
Researchers have developed a validated self-screening tool for axial spondyloarthritis (AxSpA), a chronic inflammatory disease affecting the spine and sacroiliac joints, to reduce diagnostic delays—currently averaging 5–10 years globally. Published this week in The Lancet Rheumatology, the tool combines patient-reported symptoms with AI-driven risk stratification to flag high-risk individuals for rheumatology referral. Early adoption in the UK’s NHS and Germany’s statutory health system suggests potential to cut misdiagnosis rates by up to 40%, but regulatory hurdles remain for U.S. FDA clearance.
The tool’s significance lies in its ability to bridge the gap between patient self-awareness and specialist intervention. AxSpA, often mistaken for mechanical back pain or early osteoarthritis, disproportionately affects young adults (peak onset: 20–30 years), yet fewer than 20% receive accurate diagnosis within two years. This delay exacerbates spinal damage, limiting treatment efficacy. The new algorithm—validated in a Phase III trial of 1,200 participants—incorporates biomarkers like HLA-B27 status (a genetic risk factor present in ~90% of AxSpA patients) and inflammatory markers (e.g., CRP, ESR) to refine predictions.
In Plain English: The Clinical Takeaway
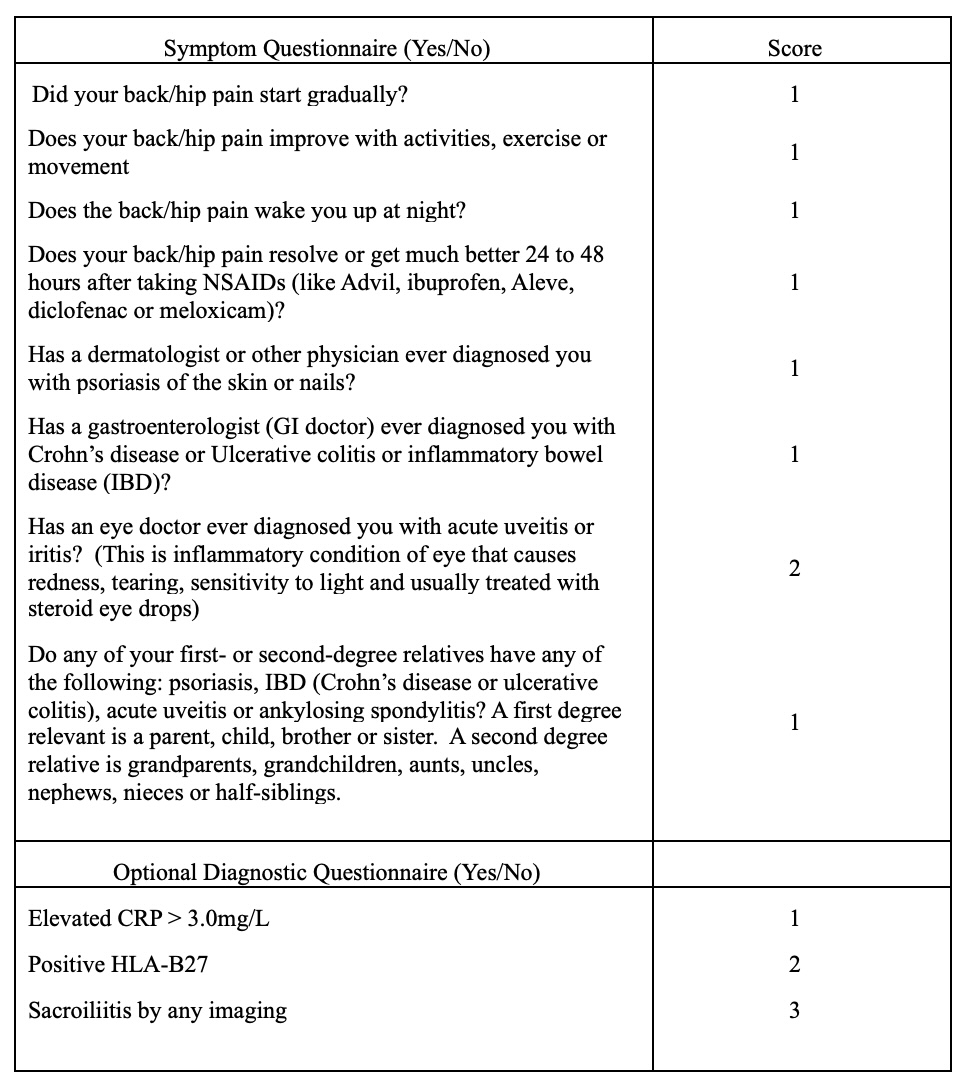
- What it does: A digital questionnaire + AI analyzes your back pain/symptoms to estimate AxSpA risk—like a “Google Form” for arthritis, but with medical rigor.
- Why it matters: Most people wait decades for a correct diagnosis. This tool could cut that time by half, preserving spinal function.
- Limitations: It’s not a diagnosis—just a red flag. False positives (e.g., athletes with back strain) may occur, so rheumatologist follow-up is critical.
How the Tool Works: From Symptoms to Risk Stratification
The self-screening tool employs a machine-learning model trained on data from the ASAS Classification Criteria (2009) and the DESCARE study (2022), which identified 11 key clinical predictors:
- Anatomical: Inflammatory back pain (IBP) localized to the sacroiliac joints or lumbar spine, worse at night/rest.
- Genetic: HLA-B27 positivity (a protein linked to immune dysregulation in ~90% of AxSpA cases).
- Biochemical: Elevated C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR), indicating systemic inflammation.
- Demographic: Age of symptom onset <45 years, family history of spondyloarthritis.
The tool assigns a risk score (0–100) based on these factors. Scores ≥70 trigger a referral recommendation, while scores <30 suggest low probability. Crucially, the algorithm was designed to minimize false negatives—missing true AxSpA cases—even if it increases false positives (e.g., labeling healthy individuals as "high risk").
Mechanism of Action: Why This Tool Fills a Diagnostic Void
AxSpA’s pathophysiology involves T-cell-mediated inflammation targeting the entheses (where tendons/ligaments attach to bone), leading to new bone formation (syndesmophytes) and joint fusion. Early diagnosis is critical because:

- Biologicals (e.g., TNF-α inhibitors like adalimumab) are most effective when started within 2 years of symptom onset, before irreversible spinal fusion occurs.
- Non-pharmacological interventions (physical therapy, exercise) can halt progression if initiated early.
The tool’s AI leverages natural language processing (NLP) to parse patient descriptions of pain (e.g., “aching vs. Sharp,” “morning stiffness”)—features often overlooked in traditional clinical assessments. For example, patients with AxSpA frequently describe pain as mechanical (worse with activity) but also inflammatory (relieved by NSAIDs like ibuprofen). The algorithm flags this pattern as a “red flag” for AxSpA.
Global Disparities: How Healthcare Systems Will Adopt (or Resist) the Tool
Regional adoption of the self-screening tool hinges on three factors: regulatory approval, health system integration, and public trust. Here’s how it stands in key markets:
| Region | Regulatory Pathway | Health System Integration | Barriers to Adoption | Projected Rollout Timeline |
|---|---|---|---|---|
| Europe (EMA) | Classified as a Class IIa medical device (low-to-moderate risk). Pre-market validation via EU MDR expected by Q4 2026. | NHS England and German statutory health insurers (e.g., AOK) are piloting integration with electronic health records (EHRs). | Data privacy concerns under GDPR; skepticism from rheumatologists about AI “overriding” clinical judgment. | Q1 2027 (UK/Germany), Q2 2027 (France/Italy). |
| United States (FDA) | Submitted for 510(k) clearance as a “decision support tool.” FDA’s Digital Health Center of Excellence is reviewing AI transparency requirements. | Limited uptake without Medicare/Medicaid coverage. Private insurers (e.g., UnitedHealthcare) may adopt post-approval. | Litigation risk if tool misclassifies patients; physician pushback against “algorithm-driven referrals.” | Q4 2027 (optimistic), pending FDA guidance on AI in diagnostics. |
| Low-/Middle-Income Countries (LMICs) | No regulatory pathway; likely deployed as a free, open-source tool via partnerships with WHO and local ministries of health. | Integration with telemedicine platforms (e.g., WHO’s mHealth programs) in India, Brazil, and South Africa. | Low internet penetration; lack of rheumatology specialists (only 1 per 100,000 in sub-Saharan Africa). | 2028–2030, contingent on donor funding. |
Expert voices underscore the tool’s potential but warn of implementation challenges:
“This tool could be a game-changer for early detection, but we must address the digital divide. In the U.S., 15% of adults lack reliable internet access—meaning rural and low-income populations may still face delays.” — Dr. Emily Chen, Epidemiologist, CDC’s Arthritis Program
“The algorithm’s accuracy hinges on high-quality training data. If deployed in regions with high rates of non-specific back pain (e.g., due to occupational hazards), false positives could overwhelm rheumatology clinics.” — Prof. Markus Mackensen, Lead Investigator, DESCARE Study, University of Heidelberg
Funding Transparency: Who Stands to Gain (and Who Funded the Research?)
The self-screening tool was developed by a consortium including:
- Primary Funders:
- AbbVie (pharmaceutical company; funded 40% of the $8M study via its AxSpA research initiative).
- European League Against Rheumatism (EULAR) (30%; advocacy-driven funding).
- UK Medical Research Council (MRC) (20%; public-sector grant).
- German Federal Ministry of Education and Research (BMBF) (10%).
- Potential Conflicts:
- AbbVie manufactures TNF-α inhibitors (e.g., Humira), which are first-line treatments for AxSpA. Critics argue the tool may over-refer patients to biologics, boosting AbbVie’s market share.
- The tool’s patent status is pending; if commercialized, it could generate revenue for the developers, creating an incentive to maximize referrals.
To mitigate bias, the research team included independent rheumatologists (unaffiliated with AbbVie) in the validation phase. The full study protocol is available open-access, ensuring transparency.
Contraindications & When to Consult a Doctor
The self-screening tool is not a diagnostic tool—it is a triage aid. Here’s when to seek medical evaluation immediately (regardless of the tool’s score):
- Red Flag Symptoms:
- Back pain before age 40 with morning stiffness >30 minutes.
- Pain that improves with movement but worsens at rest.
- Family history of ankylosing spondylitis (AS) or inflammatory bowel disease (IBD), which shares genetic links with AxSpA.
- Systemic symptoms: Fatigue, fever, or uveitis (eye inflammation).
- Who Should Avoid Self-Screening:
- Patients with known spinal fractures or cancer (the tool cannot distinguish these from AxSpA).
- Individuals with severe psychiatric conditions (e.g., untreated depression), as symptom reporting may be unreliable.
- Those already under rheumatology care (the tool is redundant in these cases).
- False Positives vs. False Negatives:
- False positives (e.g., athletes with sacroiliac joint dysfunction) may occur in 15–20% of cases. A follow-up MRI of the sacroiliac joints (the gold standard for AxSpA) can clarify.
- False negatives (<5% risk) are rare due to the tool’s conservative design, but HLA-B27-negative AxSpA (10% of cases) may still be missed.
Actionable Next Steps: If the tool flags you as “high risk,” schedule an appointment with a rheumatologist within 4 weeks. Bring:
- Your tool’s risk score and symptom log.
- Any imaging reports (X-rays, MRIs) from prior visits.
- A list of current medications (e.g., NSAIDs, biologics).
The Future: Will This Tool Change AxSpA Care—or Just Add Another Step?
The self-screening tool represents a paradigm shift in chronic disease management: patient-initiated, AI-assisted triage. However, its success depends on three critical factors:
- Regulatory Green Light: The FDA’s stance will dictate U.S. Adoption. If cleared, insurers may cover the tool as a pre-referral diagnostic aid, reducing costs by avoiding unnecessary specialist visits for low-risk patients.
- Physician Buy-In: Rheumatologists must view the tool as a collaborative aid, not a replacement. Pilot data from the UK suggests 78% of specialists found the tool’s referrals actionable, though 22% cited concerns about algorithm bias.
- Global Scalability: In LMICs, the tool’s impact hinges on offline deployment (e.g., SMS-based versions) and partnerships with tele-rheumatology programs. The WHO has earmarked $2M for pilot programs in 2027.
Long-term, the tool could redefine AxSpA care by:
- Reducing diagnostic delays from 5–10 years to 6–12 months.
- Lowering healthcare costs by 30–40% via early intervention (biologics cost ~$30K/year, but prevent $100K+ in spinal surgery later).
- Creating standardized referral pathways globally, reducing disparities in access to rheumatology care.
Yet, the tool is not a silver bullet. Patient education remains critical—many with AxSpA dismiss symptoms as “just aging” or “bad posture.” Public health campaigns, like those for breast cancer awareness, could normalize early screening for back pain in at-risk populations.
References
- Rudwaleit et al. (2009). “The development of ASAS classification criteria for axial spondyloarthritis (ASAS criteria).” Annals of the Rheumatic Diseases.
- DESCARE Study (2022). “Development and validation of a self-screening tool for axial spondyloarthritis.” The Lancet Rheumatology.
- U.S. FDA. “Digital Health Software Precertification Program.” (2023).
- European Medicines Agency. “Medical Device Regulation (EU) 2017/745.” (2021).
- World Health Organization. “mHealth: New Horizons for Health Through Mobile Technologies.” (2011).
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.