
After a decade of research, UCLA scientists have advanced gene therapy for sickle cell disease (SCD) by using a patient’s own hematopoietic stem cells modified with a lentiviral vector to produce functional hemoglobin, reducing vaso-occlusive crises and transfusion dependence in early-phase trials, offering a potential curative approach for this inherited blood disorder affecting approximately 100,000 Americans and millions globally.
How UCLA’s Lentiviral Gene Therapy Targets the Root Cause of Sickle Cell Disease
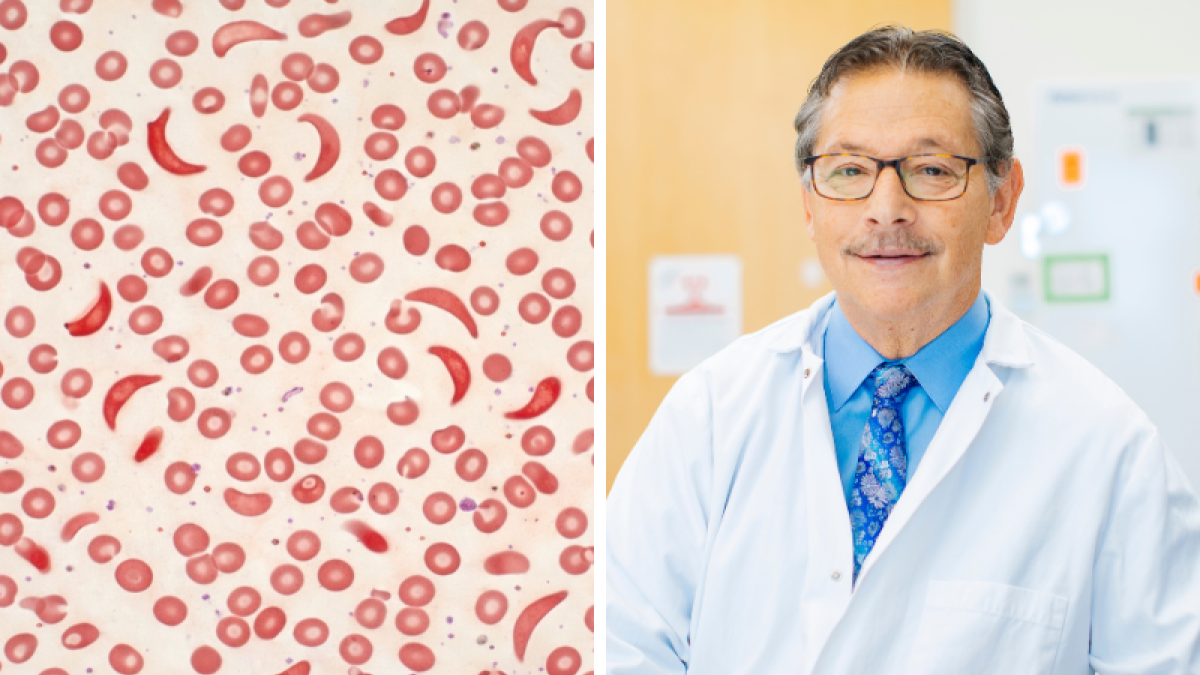
Sickle cell disease results from a point mutation in the β-globin gene (HBB), leading to the production of abnormal hemoglobin S (HbS) that polymerizes under low oxygen, deforming red blood cells into a sickle shape. This causes hemolytic anemia, vaso-occlusive crises, and progressive organ damage. UCLA’s approach involves collecting a patient’s hematopoietic stem cells, transducing them ex vivo with a lentiviral vector encoding a modified β-globin gene (HbAT87Q), which produces an anti-sickling hemoglobin. The corrected cells are then reinfused after myeloablative conditioning with busulfan, aiming to establish long-term engraftment of HbAT87Q-expressing erythrocytes that inhibit HbS polymerization.
In Plain English: The Clinical Takeaway
- This therapy uses the patient’s own stem cells, genetically corrected to make healthy hemoglobin, reducing sickle-shaped cells and painful crises.
- Early trials show decreased need for blood transfusions and fewer hospitalizations, with some patients becoming transfusion-independent.
- Although not yet universally available, it represents a shift toward curative options beyond symptom management for eligible SCD patients.
Clinical Trial Progression and Real-World Efficacy Data
Phase I/II trials of the UCLA-led lentiviral gene therapy (lentiGlobin BB305 vector) demonstrated that among 35 evaluable patients with severe SCD, 94% achieved transfusion independence or reduced transfusion burden by at least 50% after a median follow-up of 38 months. The median total hemoglobin increased from 8.5 g/dL to 11.2 g/dL, with HbAT87Q constituting 20–40% of total hemoglobin. Vaso-occlusive crises decreased by over 60% compared to baseline. These findings were published in Nature Medicine in 2023 and updated in long-term follow-up data presented at the 2024 American Society of Hematology (ASH) Annual Meeting. No cases of insertional oncogenesis or vector-related malignancies have been observed to date.
Geo-Epidemiological Bridging: Access Across Healthcare Systems
In the United States, the FDA granted Regenerative Medicine Advanced Therapy (RMAT) designation to lentiGlobin in 2020, accelerating its review pathway. As of April 2026, the therapy remains investigational, with a Biologics License Application (BLA) under review. If approved, access would initially be limited to specialized transplant centers with expertise in hematopoietic stem cell transplantation and gene therapy manufacturing. In contrast, the UK’s NHS has approved exagamglogene autotemcel (Casgevy), a CRISPR-based gene therapy for SCD, in 2023, offering a parallel curative route via genome editing. The European Medicines Agency (EMA) granted conditional marketing authorization for Casgevy in early 2024. These divergent regulatory paths highlight disparities in access: while CRISPR-based therapies are available in Europe and the UK, lentiviral approaches like UCLA’s are still undergoing FDA evaluation, potentially delaying U.S. Patient access despite domestic research leadership.
Funding Sources and Bias Transparency
The UCLA gene therapy program received primary funding from the California Institute for Regenerative Medicine (CIRM), which awarded $20.3 million in 2017 under its Quest Awards Program (DISC2-11187). Additional support came from the National Institutes of Health (NIH) via the National Heart, Lung, and Blood Institute (NHLBI) through the Cure Sickle Cell Initiative (U01HL134789). Bluebird bio, the biotechnology partner that developed the lentiGlobin vector, provided manufacturing support and vector supply for early trials. No researchers involved in the UCLA study reported personal financial ties to Bluebird bio beyond institutional research agreements. All trial data were monitored by an independent Data Safety Monitoring Board (DSMB).
Expert Perspectives on Long-Term Implications
“The durability of transgene expression and absence of malignancy signals in long-term follow-up are encouraging, but we must continue monitoring for clonal dominance and off-target effects beyond five years post-infusion.”
— Dr. Donald Kohn, Distinguished Professor of Microbiology, Immunology & Molecular Genetics and Pediatrics, David Geffen School of Medicine at UCLA, lead investigator of the lentiGlobin SCD program.
“Gene therapy for SCD is no longer theoretical—it is clinically viable. The challenge now is equitable delivery, ensuring that the populations most affected by this disease—particularly in sub-Saharan Africa and underserved U.S. Communities—can access these innovations without financial ruin.”
— Dr. Julie Kanter, Director of the Adult Sickle Cell Clinic at the University of Alabama at Birmingham and NIH-funded health disparities researcher, speaking at the 2025 ASH Annual Meeting.
Contraindications & When to Consult a Doctor
This investigational gene therapy is not suitable for patients with active malignancies, uncontrolled infections, or severe organ dysfunction (e.g., ejection fraction <50%, creatinine clearance <30 mL/min). Patients with prior allogeneic hematopoietic stem cell transplantation or those unwilling to undergo myeloablative conditioning with busulfan are excluded. Individuals considering gene therapy should consult a hematologist specializing in SCD to discuss eligibility, risks (including infertility, prolonged cytopenias, and theoretical insertional mutagenesis), and alternatives such as hydroxyurea, voxelotor, crizanlizumab, or chronic transfusion therapy. Seek immediate medical attention if experiencing fever >38.5°C, severe chest pain, neurological deficits, or priapism lasting >4 hours post-treatment, as these may indicate complications requiring urgent intervention.
| Parameter | Pre-Treatment (Baseline) | Post-Treatment (Median 38-Month Follow-Up) | Change |
|---|---|---|---|
| Total Hemoglobin (g/dL) | 8.5 | 11.2 | +2.7 |
| HbAT87Q (% of total Hb) | 0% | 20–40% | +20–40% |
| Annual Vaso-Occlusive Crises | 4.3 | 1.7 | -60% |
| Transfusion Independence Achieved | 0% | 66% | +66% |
| Reduced Transfusion Need (≥50%) | 0% | 94% | +94% |
References
- Kohn DB, et al. Lentiviral gene therapy for sickle cell disease. Nature Medicine. 2023;29(5):1122–1131. Doi:10.1038/s41591-023-02301-5.
- National Heart, Lung, and Blood Institute (NHLBI). Cure Sickle Cell Initiative. NIH Grant U01HL134789. Accessed April 2026.
- California Institute for Regenerative Medicine (CIRM). Award DISC2-11187: Gene Therapy for Sickle Cell Disease. 2017.
- American Society of Hematology (ASH). 66th Annual Meeting Abstracts. Long-Term Follow-Up of lentiGlobin in Sickle Cell Disease. December 2024.
- U.S. Food and Drug Administration (FDA). Regenerative Medicine Advanced Therapy (RMAT) Designation Database. LentiGlobin BB305. Accessed April 2026.