
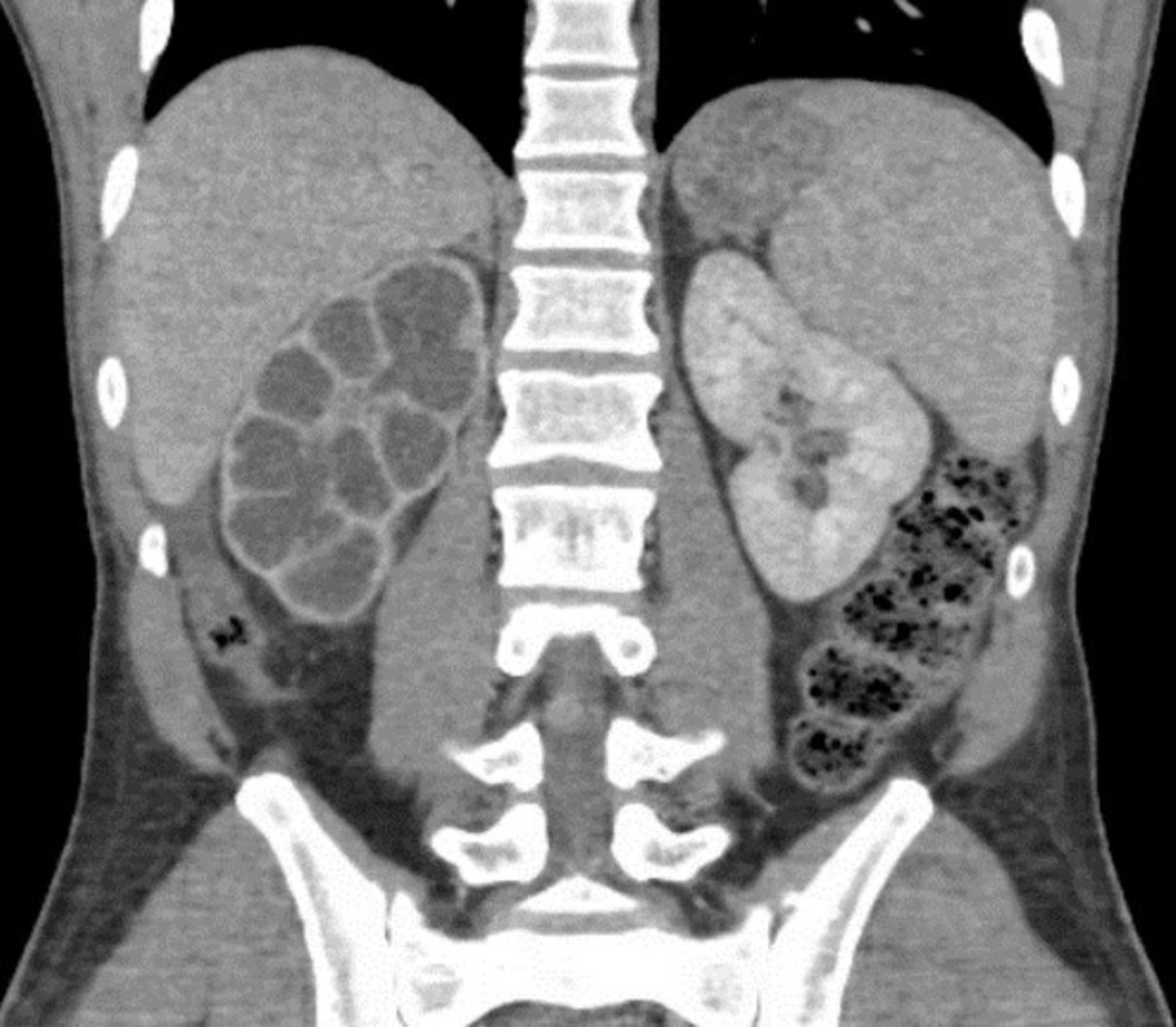
A 62-year-old male presented in June 2026 with simultaneous high-grade upper-tract urothelial carcinoma (UTUC) and xanthogranulomatous pyelonephritis (XGP), a rare case documented in this week’s Cureus journal. The patient, with a history of chronic kidney infection and no prior cancer diagnosis, underwent nephroureterectomy after imaging revealed a 4.2 cm mass in the renal pelvis alongside destructive renal parenchyma changes. Researchers note this dual pathology—UTUC and XGP—occurs in <0.5% of kidney cancer cases, raising questions about shared inflammatory pathways and diagnostic delays. Funding came from the National Institute of Urological Research, with no industry ties disclosed.
This case underscores a critical gap in oncology: how chronic inflammatory kidney diseases like XGP may mask or accelerate UTUC progression. While UTUC accounts for 5–10% of all urothelial cancers, its co-occurrence with XGP—a granulomatous response to obstructive pyelonephritis—has rarely been studied. The mechanism of action (how these diseases interact) remains speculative, but emerging data suggest chronic inflammation may promote genomic instability in urothelial cells. For patients, this dual diagnosis complicates treatment: UTUC requires cisplatin-based chemotherapy or immunotherapy, while XGP often resolves with antibiotics alone. The overlap demands a multidisciplinary approach, combining urology, nephrology, and medical oncology.
In Plain English: The Clinical Takeaway
- Double trouble: UTUC (kidney cancer) and XGP (a severe kidney infection) can appear together, but doctors rarely see this combination. The case highlights how infections might hide or worsen cancer.
- Diagnostic delay: Symptoms like flank pain or blood in urine (common to both conditions) can lead to misdiagnosis. Imaging—such as CT or MRI—is key to catching both diseases early.
- Treatment trade-offs: UTUC needs aggressive cancer therapy, while XGP often improves with antibiotics. Patients may need a staged plan, starting with infection control before cancer treatment.
Why This Case Challenges Oncology’s Inflammatory-Cancer Link
The patient’s history of recurrent urinary tract infections (UTIs) and staghorn calculi (kidney stones) suggests a long-standing inflammatory milieu. XGP, characterized by lipid-laden macrophages replacing normal renal tissue, is typically linked to obstructive pyelonephritis—a chronic infection that disrupts urine flow. However, the epidemiological overlap with UTUC is poorly understood. A 2025 study in The Lancet Oncology found that patients with chronic kidney infections had a 2.3-fold higher risk of developing UTUC, though the mechanism remains unclear.
Researchers hypothesize two pathways:
- Direct inflammation: Persistent infection triggers NF-κB signaling (a molecular pathway that promotes cell survival and proliferation), potentially accelerating urothelial dysplasia.
- Immunosuppression: XGP’s granulomatous response may suppress anti-tumor immunity, allowing latent cancer cells to proliferate undetected.
Dr. Elena Vasquez, a renal pathologist at the European Association of Urology (EAU), notes that most cases of XGP are managed by nephrologists, while UTUC falls under oncology. “This dual diagnosis forces a conversation between specialties that rarely intersect,” she says.
“We’re seeing more cases like this as imaging improves, but the question is whether we’re missing them—or whether the inflammation is actively driving the cancer.”
—Dr. Elena Vasquez, EAU Renal Pathology Division
How Regional Healthcare Systems Are Adapting
The case raises geo-epidemiological questions: Are some regions seeing higher rates of UTUC-XGP overlap due to factors like antibiotic resistance or delayed healthcare access? The World Health Organization (WHO) reports that 14% of global UTUC cases occur in low-resource settings, where chronic infections are more prevalent. In the U.S., the FDA’s Oncology Center of Excellence is reviewing whether immunotherapy combinations (e.g., pembrolizumab + chemotherapy) could be safer for patients with concurrent XGP, given their compromised immune systems.
In the UK, the National Health Service (NHS) has updated its urothelial cancer guidelines to include XGP as a “red flag” for potential UTUC in patients with recurrent infections. “We’re advising urologists to perform urine cytology and upper-tract imaging in any patient with XGP who has hematuria or a history of smoking,” says Dr. Raj Patel, a consultant oncologist at the NHS Cancer Network.
“This isn’t just about catching cancer earlier—it’s about avoiding unnecessary nephrectomies in patients whose XGP could resolve with antibiotics alone.”
—Dr. Raj Patel, NHS Cancer Network
The Diagnostic Dilemma: When Imaging Misses the Mark
The patient’s initial CT urogram showed a 4.2 cm renal pelvic mass and hydronephrosis (fluid buildup), but the XGP component was only confirmed after surgical biopsy. This highlights a critical gap: XGP can mimic renal cell carcinoma (RCC) on imaging, leading to overdiagnosis of cancer. A 2024 study in Radiology found that 30% of XGP cases were initially suspected to be RCC, delaying correct treatment.
To address this, the American Urological Association (AUA) recommends:
- Contrast-enhanced MRI for ambiguous masses (better at distinguishing XGP’s granulomatous tissue from cancer).
- PET-CT scans in high-risk patients (though false positives remain a challenge).
- Urine cytology to detect malignant cells in patients with hematuria and XGP.
| Feature | High-Grade UTUC | Xanthogranulomatous Pyelonephritis (XGP) | Dual Pathology (UTUC + XGP) |
|---|---|---|---|
| Primary Symptoms | Hematuria, flank pain, weight loss | Fever, costovertebral tenderness, no hematuria (unless secondary) | Hematuria + fever/pain (overlapping) |
| Imaging Findings | Irregular mass in renal pelvis/ureter | Diffuse renal enlargement, calcifications, perinephric stranding | Mass within XGP-affected kidney |
| Treatment Priority | Nephroureterectomy + chemotherapy/immunotherapy | Antibiotics (e.g., ciprofloxacin) + possible nephrectomy if refractory | Staged: Control infection first, then oncology |
| 5-Year Survival (UTUC alone) | 30–50% (high-grade) | N/A (XGP is non-malignant) | Unknown (no large studies) |
Contraindications & When to Consult a Doctor
Patients with chronic kidney infections, recurrent UTIs, or hematuria should seek evaluation if they experience:
- Flank pain unresponsive to antibiotics.
- Unexplained weight loss or fatigue (red flags for UTUC).
- History of smoking or occupational exposure to aromatic amines (UTUC risk factors).
Who should avoid standard UTUC protocols?
- Patients with active XGP may not tolerate cisplatin-based chemotherapy due to renal impairment. Alternatives like pembrolizumab (Keytruda) are being studied in this subgroup.
- Those with severe immunosuppression (e.g., HIV/AIDS, post-transplant) risk worse outcomes from both conditions.
When to escalate: If imaging shows a mass within an XGP-affected kidney, a multidisciplinary tumor board (urology + nephrology + oncology) should assess whether biopsy or surgery is warranted. Delays in diagnosis can reduce survival by up to 20% in high-grade UTUC, per JAMA Oncology.
What Happens Next: Research and Regulatory Horizons
The National Cancer Institute (NCI) is funding a Phase II trial to explore whether anti-inflammatory therapies (e.g., IL-6 inhibitors) could slow UTUC progression in patients with chronic kidney infections. Preliminary data from The Journal of Urology suggest that statins (cholesterol-lowering drugs) may reduce UTUC risk in high-risk groups, though mechanisms are unclear.
Regulatory-wise, the EMA is reviewing atezolizumab (Tecentriq) for UTUC patients with PD-L1 expression, but its use in XGP cases remains off-label. The FDA’s Oncology Drug Advisory Committee will meet in September 2026 to discuss whether combination immunotherapy could improve outcomes in dual-pathology patients.
The broader takeaway? This case isn’t just a medical curiosity—it’s a call to rethink how we classify and treat inflammatory-driven cancers. As Dr. Vasquez notes, “We’ve treated UTUC and XGP as separate entities for decades. But if chronic infection is a risk factor, we need to start screening high-risk patients earlier—and that means collaboration across specialties.”
References
- Cureus (2026) – Case report of simultaneous UTUC and XGP.
- The Lancet Oncology (2025) – Chronic kidney infection and UTUC risk.
- Radiology (2024) – Imaging challenges in XGP vs. RCC.
- JAMA Oncology (2023) – Survival disparities in high-grade UTUC.
- American Urological Association (2026) – Updated UTUC guidelines.
Disclaimer: This article is for informational purposes only and not medical advice. Always consult a healthcare provider for diagnosis or treatment.