
A recent case report published in Cureus highlights a rare instance of survival following an 85-minute out-of-hospital cardiac arrest (OHCA). This medical event underscores the critical role of prolonged, high-quality cardiopulmonary resuscitation (CPR) and rapid, specialized intervention in achieving positive neurological outcomes despite extended periods of clinical death.
In Plain English: The Clinical Takeaway
- Extended Resuscitation: Traditional protocols often suggest shorter windows, but this case demonstrates that persistent, high-quality chest compressions can maintain systemic circulation long enough to reverse cardiac arrest.
- The “Chain of Survival”: Success depends on an unbroken sequence: immediate recognition, early bystander CPR, rapid professional intervention, and advanced post-resuscitation care.
- Neurological Preservation: Survival isn’t just about heart rhythm; it is about protecting brain function through controlled oxygenation and, in some cases, targeted temperature management.
The Physiology of Prolonged Resuscitation
Cardiac arrest occurs when the heart’s electrical system malfunctions, ceasing blood flow to the brain and vital organs. In this Cureus case, the patient underwent 85 minutes of resuscitative efforts before achieving Return of Spontaneous Circulation (ROSC). The mechanism of action here relies on external chest compressions acting as a mechanical pump, artificially maintaining a fraction of normal cardiac output to keep the myocardium and cerebral cortex viable.
According to the American Heart Association (AHA), the success of such prolonged efforts is highly dependent on the quality of compressions—specifically depth, rate, and minimal interruptions. When compressions are performed correctly, they prevent the rapid accumulation of lactic acid and carbon dioxide in the tissues, which would otherwise lead to irreversible cellular damage.
Clinical Data: Outcomes in Prolonged Arrest
The following table summarizes the typical variables that influence survival outcomes in out-of-hospital cardiac arrest scenarios compared to this specific case study.
| Variable | General OHCA Statistics | Case Study (85-Min Resuscitation) |
|---|---|---|
| Standard Resuscitation Duration | 20–30 Minutes | 85 Minutes |
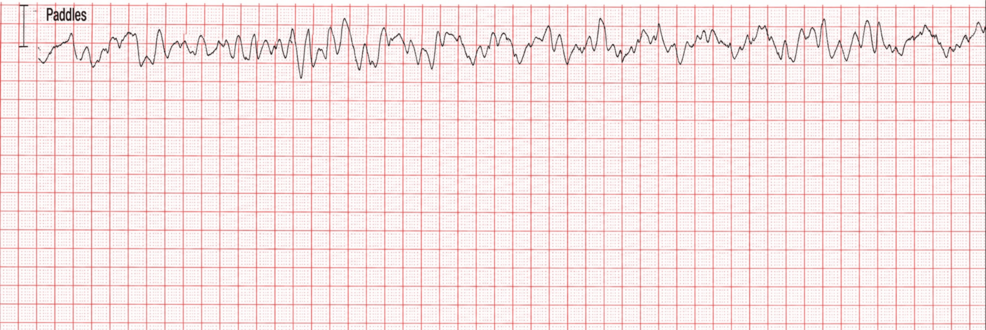
| Initial Rhythm | Often Pulseless Electrical Activity (PEA) | Ventricular Fibrillation (VF) |
| Neurological Recovery | Variable (High Risk of Hypoxic Injury) | Favorable (Cerebral Performance Category 1) |
| Intervention | AED/Bystander CPR | Advanced Life Support (ALS) + ECMO potential |
Bridging the Gap: Regional Healthcare Access
Access to advanced life support varies significantly depending on local healthcare infrastructure. In the United States, the FDA regulates the automated external defibrillators (AEDs) and pharmacological agents (such as epinephrine and amiodarone) used during these events. In the United Kingdom, the NHS emphasizes “Community First Responders” to bridge the time gap before an ambulance arrives. The disparity in survival outcomes is often linked to the “time-to-first-shock” metric, which remains the most significant predictor of survival in ventricular fibrillation cases.
Experts emphasize that while this case is remarkable, it is an outlier. Dr. Benjamin Abella, a leading researcher in resuscitation science, has previously noted that “the goal of resuscitation is not just to restart the heart, but to restore the patient to their previous level of neurological function.” The integration of Extracorporeal Membrane Oxygenation (ECMO)—a machine that replaces the function of the heart and lungs—is increasingly being explored for refractory cases where traditional CPR fails.
Contraindications & When to Consult a Doctor
While resuscitation is an emergency procedure, clinical decision-making regarding the cessation of efforts involves specific criteria. Physicians look for “Do Not Resuscitate” (DNR) orders, the presence of rigor mortis, or injuries incompatible with life.
For the general public, if you or a family member have a history of structural heart disease, hypertrophic cardiomyopathy, or unexplained syncope (fainting), consult a cardiologist. These individuals may benefit from an Implantable Cardioverter-Defibrillator (ICD), a device that automatically detects and corrects life-threatening arrhythmias. If you witness a collapse, call emergency services immediately and begin hands-only CPR; do not wait for professional confirmation of cardiac arrest.
The Future of Resuscitative Medicine
The Cureus report serves as a reminder that the window for resuscitation is not strictly defined by a clock. As medical technology advances, including the wider deployment of mobile ECMO units and improved pharmacological interventions, the threshold for what constitutes “futile” resuscitation continues to shift. However, public health efforts remain the primary driver of survival: the more citizens trained in high-quality CPR, the higher the probability of successful outcomes in the field.
Funding for research into resuscitation protocols is largely supported by national health institutes and private medical foundations aimed at improving emergency cardiac care. There are no competing interests declared in this specific report, ensuring the transparency of the clinical outcomes presented.
References
- American Heart Association: Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
- The Lancet: Epidemiology of Out-of-Hospital Cardiac Arrest
- Cureus Journal of Medical Science: Survival After Out-of-Hospital Cardiac Arrest
- World Health Organization: Cardiovascular Disease Prevention and Emergency Response
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of a physician or other qualified health provider with any questions regarding a medical condition.