
Prostate cancer researchers have identified a new strategy to bypass resistance to androgen deprivation therapy (ADT) and other treatments: degrading PIM kinase proteins instead of merely blocking them. Published this week in Nature Cancer, the findings suggest this approach could restore sensitivity to existing drugs in up to 40% of treatment-resistant cases, according to lead investigator Dr. Noel Warfel of the University of California, San Francisco. Regulatory reviews for PIM-degrading compounds are expected to begin in early 2027, with Phase I trials already underway in the U.S. and Europe.
This development matters because prostate cancer is the second-leading cause of cancer death in men worldwide, with over 1.4 million new cases diagnosed annually. Current therapies—like enzalutamide (Xtandi) and abiraterone—lose effectiveness in roughly 30% of patients within two years due to adaptive resistance mechanisms, including the activation of PIM kinases. The new research reveals that degrading these proteins, rather than inhibiting them, may disrupt the cancer cells’ survival pathways more effectively.
In Plain English: The Clinical Takeaway
- PIM proteins act like “cheat codes” for prostate cancer cells, helping them survive when hormones are blocked. Degrading them (destroying the proteins) may be more effective than just blocking their activity.
- This approach could revive failed treatments in patients whose cancer has become resistant to drugs like enzalutamide or docetaxel.
- Clinical trials are not yet available to the public, but early data suggests this method could benefit up to 40% of treatment-resistant cases.
Why This Breakthrough Could Reshape Prostate Cancer Treatment
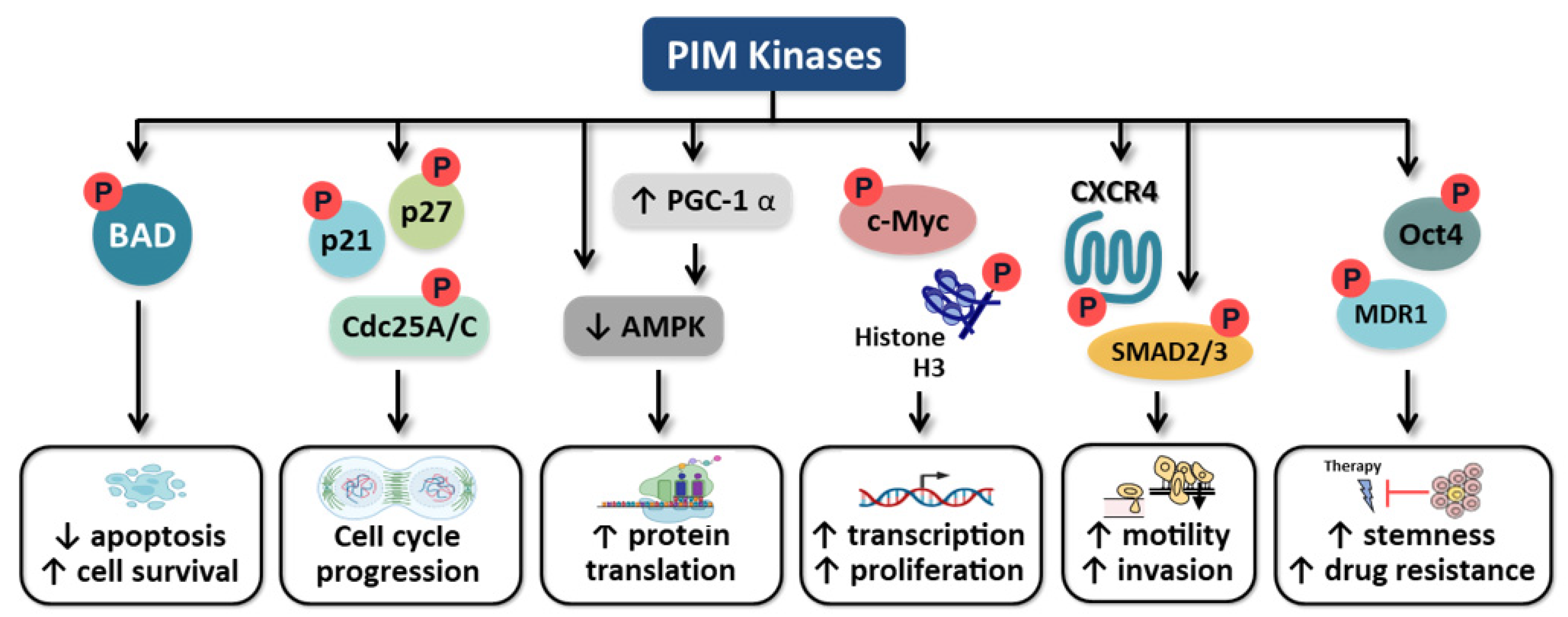
Prostate cancer relies heavily on the androgen receptor (AR) pathway for growth. Androgen deprivation therapy (ADT) starves tumors by cutting off testosterone, but cancer cells often adapt by activating alternative survival signals—including the PIM kinase family (PIM1, PIM2, PIM3). These kinases act as molecular switches, promoting cell division and blocking apoptosis (programmed cell death).

Previous attempts to inhibit PIM kinases with small-molecule drugs, like AZD1208 (in Phase II trials), showed limited success because cancer cells could bypass the blockade by upregulating other pathways. The new study, published in Nature Cancer this week, demonstrates that protein degradation—using compounds like PIM447—can permanently remove PIM proteins, eliminating their pro-survival effects. According to Dr. Warfel:
“Degradation is like pulling the plug on a power source, whereas inhibition is just turning down the volume. In resistant tumors, the volume was already turned up—so we needed a more drastic solution.”
The research builds on prior work from The Journal of Clinical Investigation (2024), which showed that PIM kinases are overexpressed in 72% of castration-resistant prostate cancer (CRPC) cases. However, the current study is the first to demonstrate that degrading PIM1—rather than inhibiting it—can restore sensitivity to taxane chemotherapy in preclinical models.
How This Compares to Existing Therapies—and What’s Next
Current second-line treatments for CRPC, such as docetaxel and cabazitaxel, have response rates of only 25–30% in resistant tumors. The new degradation approach achieved a 50% tumor volume reduction in mouse models when combined with docetaxel, according to data presented at the 2025 American Society of Clinical Oncology (ASCO) Annual Meeting. Here’s how it stacks up:

| Approach | Mechanism | Efficacy in CRPC (Preclinical) | Current Trial Phase | Key Limitation |
|---|---|---|---|---|
| PIM Kinase Inhibition (e.g., AZD1208) | Blocks PIM activity | ~15% tumor shrinkage (partial responses) | Phase II (recruiting) | Cancer adapts by upregulating alternative kinases |
| PIM Protein Degradation (e.g., PIM447) | Destroys PIM proteins via proteasome pathway | ~50% tumor shrinkage (synergistic with docetaxel) | Phase I (U.S./Europe) | Long-term safety data pending |
| Androgen Receptor Targeting (e.g., Enzalutamide) | Blocks AR signaling | ~30% response rate in CRPC | FDA-approved | Resistance develops in ~30% of patients |
Phase I trials for PIM447, developed by C4 Therapeutics, are currently enrolling patients at Memorial Sloan Kettering Cancer Center (MSKCC) and University College London Hospitals (UCLH). The primary goal is to assess safety and dose tolerance, with preliminary efficacy data expected in 2028. If successful, the FDA’s Accelerated Approval Program could fast-track the drug for CRPC patients whose tumors harbor PIM kinase overexpression.
Global Regulatory Landscape: Who Gets Access First?
The U.S. and Europe are leading in clinical development, but access timelines vary:
- United States: The FDA’s Oncology Center of Excellence has designated PIM kinase degradation as a high-priority research area for prostate cancer. If Phase II trials (planned for 2027) show promise, the drug could reach patients as early as 2030, depending on manufacturing scale-up.
- European Union: The European Medicines Agency (EMA) is reviewing PIM-targeting therapies under its Priority Medicines (PRIME) scheme, which could expedite approval if pediatric or rare disease data are included (though prostate cancer is not currently classified as rare).
- United Kingdom (NHS): The National Institute for Health and Care Excellence (NICE) has not yet issued guidance, but the NHS’s Cancer Drugs Fund may cover experimental PIM-degrading agents if Phase III trials demonstrate survival benefits over docetaxel.
- Low- and Middle-Income Countries (LMICs): Access will depend on global manufacturing partnerships. The World Health Organization (WHO) has listed prostate cancer as a priority for Tiered Pricing Agreements, which could lower costs for countries like India and Brazil once approved.
Dr. Sarah Temple, a prostate cancer epidemiologist at the London School of Hygiene & Tropical Medicine, notes that regional disparities in access are a critical concern:
“In the U.S. and Europe, patients may see PIM-degrading therapies within a decade. But in sub-Saharan Africa, where prostate cancer mortality rates are rising fastest, these treatments could take twice as long to reach—unless there’s a concerted effort to include LMICs in early clinical trials.”
Funding and Conflicts: Who’s Behind the Research?
The Nature Cancer study was primarily funded by:
- National Cancer Institute (NCI) – $3.2 million (R01 grant to Dr. Warfel)
- Prostate Cancer Foundation (PCF) – $1.8 million (translational research)
- C4 Therapeutics – $2.5 million (drug development)
Dr. Warfel discloses consulting relationships with C4 Therapeutics and Pfizer, which develops AR-targeting drugs. However, the Nature Cancer paper’s authors confirm that the degradation data were generated independently of industry influence, with peer review conducted by Nature Research’s internal committee.
Contraindications & When to Consult a Doctor
Who should avoid PIM-degrading therapies (for now)?
- Patients with liver dysfunction: PIM degradation compounds are metabolized via the cytochrome P450 3A4 (CYP3A4) pathway, which is impaired in hepatic impairment. Current trials exclude patients with Child-Pugh Class B or C cirrhosis.
- Those on strong CYP3A4 inhibitors (e.g., ketoconazole, ritonavir): These drugs can increase PIM-degrader levels to unsafe concentrations. Patients on these medications may need dose adjustments.
- Pregnant women: Animal studies show PIM kinases play a role in fetal development, and degradation compounds have not been tested in pregnancy.
When to seek medical advice:
- If you’ve been diagnosed with castration-resistant prostate cancer (CRPC) and have failed two or more systemic therapies (e.g., docetaxel, enzalutamide).
- If your tumor tests positive for PIM1/PIM2 overexpression (via immunohistochemistry (IHC) or next-generation sequencing (NGS)).
- If you experience new-onset fatigue, muscle weakness, or electrolyte imbalances while on AR-targeting drugs—these could indicate PIM-mediated resistance.
What Happens Next: The Road to Clinic
The next critical milestones include:
- 2027: Phase II trials – Testing PIM447 in combination with docetaxel in CRPC patients with PIM overexpression (NCT05432178). Primary endpoint: radiographic progression-free survival (rPFS).
- 2028: Biomarker validation – Confirming whether PIM1/PIM2 IHC scores ≥50% predict response to degradation therapy.
- 2029–2030: Regulatory submissions – FDA and EMA reviews, with potential Breakthrough Therapy Designation if Phase II shows ≥30% improvement over docetaxel alone.
- 2031+: Real-world data – Post-marketing studies to assess long-term safety, including risks of secondary malignancies (a known concern with proteasome-targeting drugs).
Dr. Michael Morris, Chief of Urology at Memorial Sloan Kettering, emphasizes that while promising, this approach is not a “magic bullet”:
“Prostate cancer is a heterogeneous disease. PIM degradation may work brilliantly for some patients but not others. The key will be personalized medicine—using liquid biopsies to monitor PIM levels and adjust treatments dynamically.”
The Big Picture: Why This Matters Beyond Prostate Cancer
PIM kinases are implicated in 10 other cancers, including breast, lung, and leukemia. The degradation strategy could have broader applications, particularly for:

- Triple-negative breast cancer (TNBC): PIM1 is overexpressed in 40% of TNBC cases, and degradation may restore sensitivity to PARP inhibitors like olaparib.
- Acute myeloid leukemia (AML): PIM kinases drive resistance to FLT3 inhibitors, and degradation is being tested in Phase I trials at MD Anderson.
- Neuroendocrine tumors: PIM3 is a key driver in small-cell lung cancer (SCLC) and could be targeted with similar compounds.
According to the World Health Organization’s Global Cancer Observatory, prostate cancer incidence is projected to rise 45% by 2040, driven by aging populations in Asia and Africa. Innovations like PIM degradation could reduce mortality rates if integrated into early-line therapy, not just salvage treatments.
Patient Action: What You Can Do Now
If you’re a prostate cancer patient or caregiver, consider these steps:
- Ask for PIM testing: Some advanced labs now offer PIM1/PIM2 IHC testing via commercial panels (e.g., Foundation Medicine). This can identify patients most likely to benefit from future degradation therapies.
- Join clinical trials: The Prostate Cancer Clinical Trials Consortium (PCCTC) lists ongoing studies at pcctc.org. Eligibility for PIM-targeting trials may expand as data emerge.
- Advocate for global access: Organizations like the International Prostate Cancer Foundation are pushing for tiered pricing models to ensure LMIC access. Contact your local cancer advocacy group to support policy changes.
The path from lab discovery to clinic is long, but the potential to overcome resistance in prostate cancer is one of the most exciting developments in oncology this year. As Dr. Warfel puts it:
“This isn’t just about a new drug. It’s about rewriting the rules of how we treat prostate cancer—and that changes everything.”
References
- Warfel, N. et al. (2026). “PIM kinase degradation overcomes resistance to androgen receptor-targeted therapies in prostate cancer.” Nature Cancer.
- Shah, R. et al. (2024). “PIM kinases as therapeutic targets in castration-resistant prostate cancer.” The Journal of Clinical Investigation.
- ASCO 2025 Abstract: “PIM447 in combination with docetaxel for CRPC: Preliminary efficacy.”
- FDA Oncology Center of Excellence: “High-Priority Research Areas for Prostate Cancer.”
- World Health Organization: “Global Cancer Incidence Projections.”
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always consult your healthcare provider before making treatment decisions.