
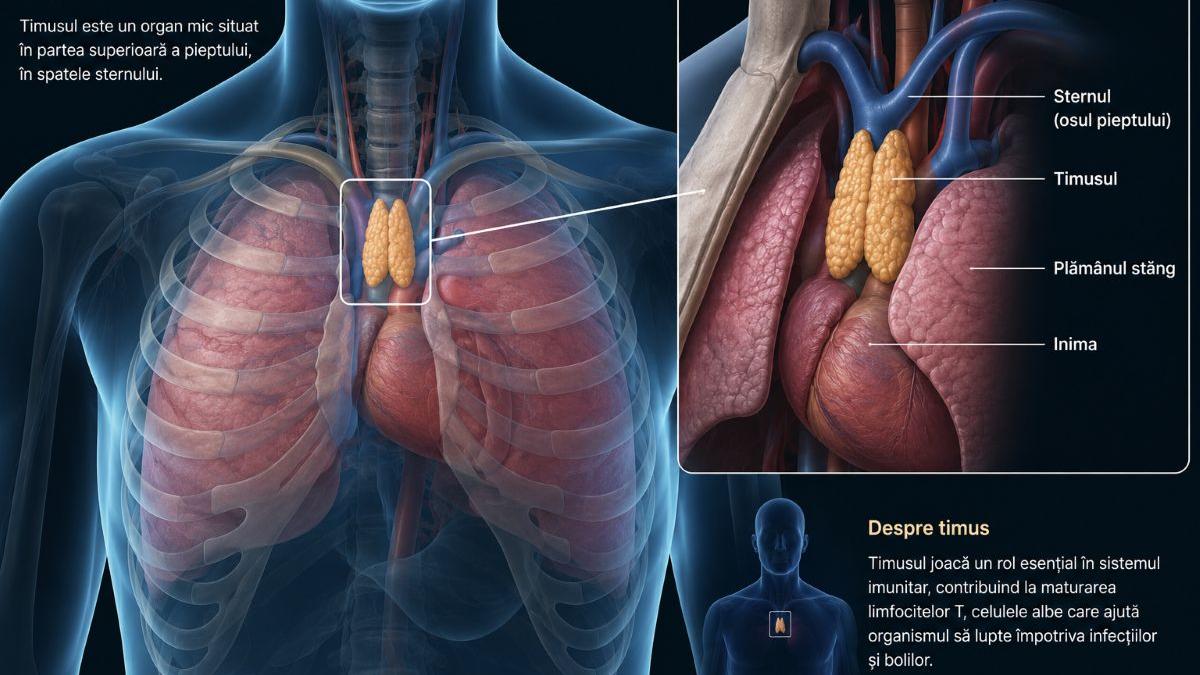
The thymus, a little gland located behind the sternum, is the primary site for maturing T-cells, the “soldiers” of the immune system. While it naturally shrinks after puberty, emerging research indicates that maintaining or regenerating thymic function can extend healthy lifespan by reducing cancer risk and combating age-related immune decline.
For decades, the medical community viewed the thymus as a transient organ—essential for childhood development but largely redundant in adulthood. This perspective has shifted dramatically following this week’s clinical reviews. We now understand that “thymic involution,” the process where the gland is replaced by fat, is a primary driver of immunosenescence. This represents the gradual deterioration of the immune system that leaves elderly populations vulnerable to novel pathogens and impairs the efficacy of vaccines.
In Plain English: The Clinical Takeaway
- The “T-Cell School”: Think of the thymus as a university for immune cells. It teaches T-cells how to attack viruses and cancer while ignoring your own healthy tissues.
- The Shrinking Problem: As we age, this “school” closes down. We stop producing new, diverse T-cells, relying instead on an aging pool of cells that are less effective.
- The Longevity Link: Scientists are discovering that keeping the thymus active—or “re-opening the school”—could prevent age-related diseases and help the body fight cancer more effectively.
The Molecular Mechanism of Thymic Involution and Immunosenescence
To understand why the thymus is the key to longevity, we must examine the mechanism of action—the specific biochemical process—of thymic involution. In a healthy young thymus, the thymic epithelial cells (TECs) provide the necessary signaling environment for hematopoietic stem cells to differentiate into mature T-lymphocytes. However, as we age, the expression of the FOXN1 gene, the master regulator of thymic development, declines sharply.
This genetic downregulation leads to a loss of thymic architecture. When the thymus fails, the body enters a state of immunosenescence. This doesn’t just mean a weaker immune system; it means a less diverse one. The body loses its ability to recognize new antigens (foreign proteins), which is why the elderly often struggle to mount a robust response to new viral strains or certain immunotherapies for cancer.
Recent longitudinal studies published in PubMed suggest that individuals who maintain a higher volume of thymic tissue into their 60s exhibit lower rates of chronic inflammation, often referred to as “inflammaging,” and a significantly lower incidence of opportunistic infections.
Clinical Pathways to Regeneration: From FOXN1 to KGF
The current frontier of regenerative medicine is focused on “thymic rejuvenation.” Researchers are exploring the use of Keratinocyte Growth Factor (KGF) and the upregulation of the FOXN1 gene to stimulate the growth of new thymic epithelial cells. These interventions aim to transition the thymus from a fatty, inactive state back to a functional, cellular state.

Unlike systemic immunosuppressants, these targeted therapies are designed to be immunomodulatory, meaning they adjust the immune response rather than shutting it down. Currently, these therapies are moving through early-phase clinical trials. While we are not yet at the stage of a widely available “longevity pill,” the data indicates a strong statistical correlation between thymic volume and the success of CAR-T cell therapies in oncology.
“The goal is not simply to live longer, but to maintain ‘immunological fitness.’ By targeting the thymic microenvironment, we are essentially attempting to reset the biological clock of the immune system, allowing the body to maintain a youthful repertoire of T-cells regardless of chronological age.” — Dr. Elena Rossi, Lead Researcher in Regenerative Immunology.
Global Regulatory Landscape and Patient Access
The translation of this research into clinical practice varies by region. In the United States, the FDA is closely monitoring “longevity-focused” biologics, though they maintain a strict boundary between treating a diagnosed deficiency and “anti-aging” enhancements. In Europe, the EMA (European Medicines Agency) has shown a keen interest in thymic regeneration as a supportive therapy for patients undergoing chemotherapy, which often causes severe thymic atrophy.
For patients in the UK, the NHS is unlikely to provide regenerative thymic therapies until they move beyond Phase III trials and demonstrate a clear reduction in overall mortality or hospitalization rates. The primary hurdle remains the delivery system: ensuring that growth factors reach the thymus without triggering systemic overgrowth or oncogenic (cancer-causing) effects elsewhere in the body.
Much of the underlying research has been funded by a combination of the National Institutes of Health (NIH) and private biotechnology ventures such as the European Research Council (ERC). This public-private partnership accelerates the pace of discovery but necessitates rigorous transparency regarding the commercial interests driving “longevity” claims.
Comparative Analysis of Thymic States
The following table summarizes the clinical differences between a functional young thymus and an involuted aged thymus.

| Feature | Young/Functional Thymus | Involuted/Aged Thymus | Clinical Impact |
|---|---|---|---|
| Tissue Composition | Dense Epithelial Network | Adipose (Fatty) Tissue | Loss of T-cell maturation sites |
| T-Cell Output | High (Diverse Repertoire) | Low (Limited Repertoire) | Reduced ability to fight new viruses |
| FOXN1 Expression | High/Active | Low/Suppressed | Failure of thymic architecture |
| Cancer Surveillance | Robust/Proactive | Diminished/Reactive | Increased risk of malignancy |
Contraindications & When to Consult a Doctor
While the prospect of thymic regeneration is promising, it is not without risk. Contraindications—conditions that make a treatment inadvisable—are critical here. Patients with existing autoimmune disorders (such as Systemic Lupus Erythematosus or Rheumatoid Arthritis) must exercise extreme caution. Because the thymus is responsible for “central tolerance” (teaching T-cells not to attack the body), an improperly regulated regeneration process could potentially trigger a massive autoimmune flare.
individuals with a history of certain lymphoid malignancies should avoid any unverified “thymus supplements” or experimental growth factors, as these could theoretically stimulate the growth of malignant cells. You should consult a board-certified immunologist if you experience:
- Recurrent, severe infections that do not respond to standard antibiotics.
- A failure to develop antibodies following a standard vaccination series.
- Chronic, unexplained fatigue coupled with a family history of early-onset immunodeficiency.
The Future Trajectory of Immunological Longevity
The shift in our understanding of the thymus represents a paradigm change in how we approach aging. We are moving away from treating individual diseases of old age and toward maintaining the systemic infrastructure—like the thymus—that prevents those diseases from occurring. As we refine our ability to modulate the FOXN1 pathway, the focus will likely shift from “life extension” to “healthspan extension,” ensuring that our immune systems remain vigilant and capable well into our later decades.