
{kind=link}
Thyroid Nodule Treatment: Study Compares Surgery and Laser Ablation
Table of Contents
- 1. Thyroid Nodule Treatment: Study Compares Surgery and Laser Ablation
- 2. Study Design and Patient Selection
- 3. Laboratory Workup
- 4. Thyroid Ultrasound
- 5. Surgical Technique
- 6. Laser Ablation
- 7. Understanding Thyroid Nodules: A Basic Overview
- 8. Frequently Asked Questions About Thyroid Nodules
- 9. What are the key factors to consider when choosing between thyroid nodule surgery and ablation?
- 10. Thyroid nodule Treatment: Surgery vs. Ablation
- 11. Understanding Thyroid Nodules
- 12. Thyroid Nodule Surgery (Thyroidectomy)
- 13. When is Thyroidectomy Recommended?
- 14. Thyroidectomy: Advantages and Disadvantages
- 15. Thyroid Nodule Ablation: A Minimally Invasive Approach
- 16. Radiofrequency Ablation (RFA)
- 17. Ethanol Ablation
- 18. Ablation: Advantages and Disadvantages
- 19. Comparing Surgery and Ablation: Which is Right for You?
- 20. Practical Tips and Considerations
A New Study Conducted In Poland Evaluated Different Treatment Options For Asymmetric Thyroid Nodules. The Research Compared Surgical Procedures And Laser Ablation (LA) To Determine Patient Preferences And Treatment Outcomes.
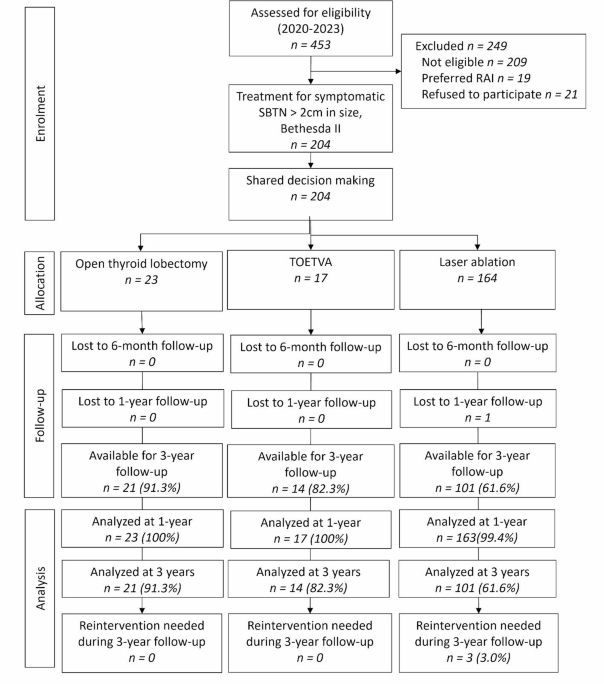
The Study, Performed At The Thyroid Disease Treatment Center In krakow, Registered Patients between January 2020 and December 2023.The focus was On Patients With A Solitary Benign Thyroid Nodule (SBTN) On One Side Of The Thyroid, With The Other Lobe Appearing Normal On Ultrasound.
Researchers Adhered To The Declaration Of Helsinki Principles. The Bioethics Committee Of The Jagiellonian University Granted Approval For The Study.
Study Design and Patient Selection
Eligible Patients With An Asymmetric Nodular Goiter Underwent Assessment For This Prospective Cohort Study. Inclusion Criteria Included A SBTN With The Contralateral Thyroid Lobe Appearing Normal On Ultrasound, In An Euthyroid Patient, Nodule Volume ≥ 5 Ml, Spongiform, Predominantly Solid (Solid Portion > 80%), Or Solid Nodule, Compression Symptoms Or Cosmetic Concerns, Confirmation Of A benign Thyroid Nodule In two Fnas, Normal Calcitonin Serum Level With The Absence Of Antithyroglobulin Antibodies (Tgab) And Antithyroid Peroxidase Antibodies (Tpoab), or A Solitary Autonomously Functioning Thyroid Nodule (AFTN) < 10 Ml In A Patient Refusing Radioactive Iodine (Rai) treatment.
Exclusion Criteria Included: Multinodular/Bilateral Euthyroid Or Toxic Goiter, Nodules Showing Ultrasonographic Features Suggestive High Risk Of Malignancy (Eu-Tirads 5), Previous Thyroid Surgery Or Nodule Treatment, Pregnancy Or Lactation, Age < 18 Years, Asa 4 Grade (American Society Of Anesthesiology), And Inability To Comply With The Follow-Up Protocol.
Ultimately,204 Eligible Patients Were Offered The Choice Between Surgery (Open Lobectomy Or Toetva) And La. This Was Based On their Preferences after Shared Decision-Making (Sdm). Patients Signed Informed Consent Forms and Were Scheduled For Treatment Within four Weeks.
the Primary Focus Of The Study Was Patient Treatment Preferences. Secondary Areas Of Focus Included Success Rates, Overall Morbidity, The Need For Additional Treatment, And patient Satisfaction.
Success Rate Was Defined As A Nodules Volume Reduction Of More Than 50% After One Year. This Was Measured By Both Technical success Rate And The Relief Of Compression Symptoms, Which Was Measured By Clinical Success Rate.
Pretreatment And Posttreatment Laryngoscopy Were Mandatory For All Patients Undergoing Surgery. It Was Also Recommended For Patients Experiencing Voice Changes After La.
Laboratory Workup
Serum Tsh, Free T4 (Ft4), Thyroglobulin (Tg), Tpoab, Tgab, And Calcitonin Levels Were Assessed Before Treatment. These levels Were Then Assessed Annually After The Treatment.
Thyroid Ultrasound
Thyroid Ultrasound Evaluation Was Performed By The Same Physician (M.B. Or J.B.) At Baseline. Commercially Available Ultrasound Machine (Voluson P8, Ge, San jose, Ca, Usa) Was Used. Nodule Volume Was Reported In ml Using The Following Ellipsoid Volume Formula: (Length × Width × Depth) × 0.53.
Nodules Were Classified As Spongiform, Solid, Or Predominantly Solid Based On Their Composition. Nodules Were Classified Based On Their Size As Small (≤ 10 ml), Medium (10-30ml), And Large (> 30 Ml).
Surgical Technique
Surgical Operations Were Performed Under General Anesthesia With Endotracheal Intubation And Neuromonitoring. All Total Extracapsular Unilateral Thyroid Lobectomies Were Performed By The Same Experienced Endocrine Surgeon (M.B.).
The Surgeon Used Either Open Technique Or Toetva. In Each Patient, The Ipsilateral Recurrent Laryngeal Nerve Was Exposed. The Parathyroid Glands Were Meticulously Dissected From The Thyroid Gland, And Effort Was Made To Identify Both Ipsilateral Parathyroid Glands And Preserve Them “In Situ”.
Contralateral Thyroid Disease Was excluded Preoperatively By Ultrasonography Of The Neck. An Overnight Hospital Stay Was Mandatory For All Patients Undergoing Surgery.
Laser Ablation
Two Operators, An Experienced Endocrine Surgeon (M.B.) And Endocrinologist (J.B.),Performed all Laser Ablation Procedures. Patients Were Placed Supine With Their Neck Fully Extended.
After An Ultrasound Examination Of The Neck And Planning Of The Entry Point Of The Needles, Local Anesthesia Was Administered.
Understanding Thyroid Nodules: A Basic Overview
Thyroid nodules Are Common Growths That Develop Within The Thyroid Gland. Most Are Benign, But Some Can Be Cancerous, Requiring further Evaluation And Treatment. Regular check-Ups And Monitoring Are Essential For Managing Thyroid health.
Treatment Options Vary Depending On The Nodule Size, Symptoms, And Whether It Is Cancerous. Options Range from Active Surveillance To Surgery Or Minimally Invasive Procedures Like Laser Ablation.
Frequently Asked Questions About Thyroid Nodules
- What is asymmetric nodular goiter?
Asymmetric Nodular goiter Refers To An enlargement of The Thyroid Gland Where Nodules Are Primarily Located On One Side,causing An Uneven Appearance.
- What were the primary endpoints of the thyroid nodule treatment study?
The Primary Endpoint Was Patient Preference For Treatment. Secondary Endpoints Included Success Rate, Overall Morbidity, Need For Second-Line Treatment, And Satisfaction Rate.
- How was success rate defined in the thyroid nodule treatment study?
Success Rate Was Defined as The Proportion Of Nodules With More Than 50% Reduction In Volume At 12 Months (Technical Success Rate) And Relief Of Compression Symptoms (Clinical Success Rate).
- what surgical techniques were used in the thyroid nodule treatment study?
The Surgical Operations Included Total Extracapsular Unilateral thyroid Lobectomies Performed Using either Open Technique Or Transoral Thyroid Lobectomy By Vestibular Approach (TOETVA).
- What is laser ablation for thyroid nodules?
Laser Ablation Is A Minimally Invasive Procedure Where Laser Energy Is Delivered To The Thyroid Nodule To Reduce Its Size. It Was Performed By Experienced Professionals.
- What were the inclusion criteria for the thyroid nodule treatment study?
Inclusion Criteria Included A Solitary Benign Thyroid Nodule (SBTN) With A Normal Contralateral Lobe, Euthyroid Status, Nodule Volume ≥ 5ml, Confirmation Of Benignity In Two FNAs, And Normal Calcitonin Levels.
- What is TOETVA?
TOETVA Stands For transoral Endoscopic Thyroidectomy Vestibular Approach. It is a minimally invasive surgical technique where the thyroid is accessed through the mouth.
What Are Your Thoughts On These Thyroid Nodule Treatment Options? Share Your Comments And Questions Below.
disclaimer: This Article Provides General Facts And Should not Be Considered Medical Advice. Consult With A Qualified Healthcare Professional For Diagnosis And Treatment Of Thyroid Conditions.
What are the key factors to consider when choosing between thyroid nodule surgery and ablation?
Thyroid nodule Treatment: Surgery vs. Ablation
Dealing with thyroid nodules can be complex. Understanding your treatment options is crucial for making informed decisions about your thyroid health. This guide compares two popular methods: thyroid nodule surgery (thyroidectomy) and thyroid ablation, focusing on Radiofrequency Ablation (RFA) and other ablation techniques. We will delve into the pros and cons of each based on various factors, including nodule size, nodule characteristics (benign or malignant), and overall patient health.
Understanding Thyroid Nodules
Thyroid nodules are lumps that form within the thyroid gland. They’re incredibly common, with many people not even realizing they have them. The NDR.de website (provided as web search result) highlights that thyroid nodules can sometimes cause no symptoms, but can also be associated with thyroid dysfunction.
These lumps can be:
- Benign (non-cancerous): These are the most common type.
- Malignant (cancerous): Less common,but require prompt treatment.
- Indeterminate: Nodules where it is not clearly persistent if they are benign or malignant may require additional testing such as a biopsy.
Your endocrinologist will conduct tests, including a thyroid ultrasound and potentially a fine needle aspiration (FNA) biopsy, to determine the nature of the nodules. These tests are crucial for guiding treatment decisions.
Thyroid Nodule Surgery (Thyroidectomy)
Thyroidectomy, or thyroid surgery, involves the surgical removal of all or part of the thyroid gland.It’s a well-established treatment option, but it’s also an invasive procedure.
When is Thyroidectomy Recommended?
Surgery is often recommended in the following scenarios:
- suspicious or cancerous nodules: To remove the nodule and potentially the entire gland to prevent further spread.
- Large nodules causing compression: Nodules that are compressing the trachea (windpipe) or esophagus (food pipe) can make swallowing or breathing difficult.
- Hyperthyroidism due to a nodule: If a nodule is producing excess thyroid hormone,leading to hyperthyroidism.
Thyroidectomy: Advantages and Disadvantages
Let’s compare the key aspects in a table for ease of understanding:
| Advantages | disadvantages |
|---|---|
| Effective for both cancerous and benign nodules. | Invasive procedure, requiring general anesthesia. |
| Provides a definitive diagnosis through pathological examination. | Risk of complications: bleeding, infection, damage to the recurrent laryngeal nerve (voice changes), hypoparathyroidism (low calcium). |
| Can resolve compressive symptoms. | Requires a scar on the neck. |
| Might potentially be curative for thyroid cancer. | Requires lifelong thyroid hormone replacement therapy (if the entire thyroid is removed). |
Thyroid Nodule Ablation: A Minimally Invasive Approach
Thyroid ablation is a less invasive treatment option compared to surgery. It involves destroying the nodule without removing the thyroid gland. The most common types of ablation are radiofrequency ablation (RFA) and ethanol ablation.
Radiofrequency Ablation (RFA)
RFA is a minimally invasive procedure that uses radiofrequency energy to heat and destroy the nodule. It’s typically performed on an outpatient basis.
How RFA Works:
- A thin needle is guided into the nodule using ultrasound.
- Radiofrequency energy is delivered through the needle, creating heat.
- The heat destroys the nodule tissue.
Ethanol Ablation
Also known as percutaneous ethanol injection (PEI),this method involves injecting ethanol (alcohol) directly into the nodule. This causes the nodule tissue to die off. PEI is used less frequently than RFA for thyroid nodules.
Ablation: Advantages and Disadvantages
Here’s a table comparing the advantages and disadvantages of thyroid Ablation:
| Advantages | Disadvantages |
|---|---|
| Minimally invasive, often performed on an outpatient basis. | May not be suitable for cancerous nodules.(Considered a controversial therapy based on pathology and size) |
| Generally fewer complications than surgery. | Nodules can sometimes regrow, requiring repeat treatments. |
| Preserves thyroid function in many cases. | Potential for temporary soreness or swelling. |
| No scar. | Less experience than surgery. |
Comparing Surgery and Ablation: Which is Right for You?
The best treatment for your thyroid nodule depends on several factors. Your doctor will consider the following:
- Nodule Size: Larger nodules may be better suited for surgery, especially if they’re causing compressive symptoms.
- nodule Characteristics: Surgery is often preferred for suspicious or cancerous nodules.
- Patient Health: Ablation may be a better option for patients who are not good candidates for surgery due to other health issues.
- Patient Preference: The patient’s wishes and lifestyle play a role.
Here’s a simplified comparison:
| Feature | Surgery (Thyroidectomy) | Ablation (RFA/Ethanol) |
|---|---|---|
| Invasiveness | High | Low |
| Recovery Time | Longer | Shorter |
| Scarring | Yes | No |
| Effectiveness (Cancerous Nodules) | Generally more effective | Less effective (not usually recommended) |
| thyroid Hormone Replacement | often Required (If total thyroidectomy) | Rarely needed. |
Practical Tips and Considerations
- Second Opinion: always seek a second opinion from another endocrinologist or surgeon to confirm your diagnosis and treatment plan.
- Research Your Doctor: Choose an experienced doctor who specializes in thyroid conditions.
- Ask Questions: Don’t hesitate to ask your doctor any questions you have about the procedure, the risks, and the expected outcomes.
- Follow-Up Care: Ensure you understand the importance of regular follow-up appointments to monitor your thyroid health after treatment.
disclaimer: This article provides general information and does not substitute for professional medical advice. Always consult with your doctor or qualified healthcare professional before making any decisions about your health or treatment.