
A recent case report published this week in Cureus details a patient with undiagnosed HIV who presented with tuberculosis (TB) peritonitis. This rare extrapulmonary manifestation of TB underscores the critical need for early HIV screening in patients presenting with atypical abdominal symptoms to ensure timely, life-saving intervention.
This case is a sobering reminder that the intersection of HIV and tuberculosis remains one of the deadliest synergies in global health. When a patient is unaware of their HIV status, their immune system—specifically the CD4+ T-lymphocytes—is depleted, leaving them vulnerable to opportunistic infections. In this instance, Mycobacterium tuberculosis did not just settle in the lungs but migrated to the peritoneum (the lining of the abdominal cavity), creating a complex clinical picture that mimics other forms of abdominal distress.
In Plain English: The Clinical Takeaway
- The Hidden Link: HIV weakens the immune system, making it easier for TB to spread from the lungs to other organs, like the abdomen.
- The Diagnostic Trap: Abdominal TB can look like other diseases (such as cancer or appendicitis), meaning doctors must specifically test for TB and HIV to get the right diagnosis.
- The Urgency: Early detection of both HIV and TB is vital; treating TB without addressing HIV (or vice versa) can lead to poor outcomes.
The Pathophysiology of Extrapulmonary Dissemination
In a healthy immune system, the body contains Mycobacterium tuberculosis within granulomas—slight, walled-off clusters of immune cells that prevent the bacteria from spreading. However, in patients with advanced HIV, the “mechanism of action” (the specific way a biological process works) changes. The depletion of CD4+ cells leads to the breakdown of these granulomas.
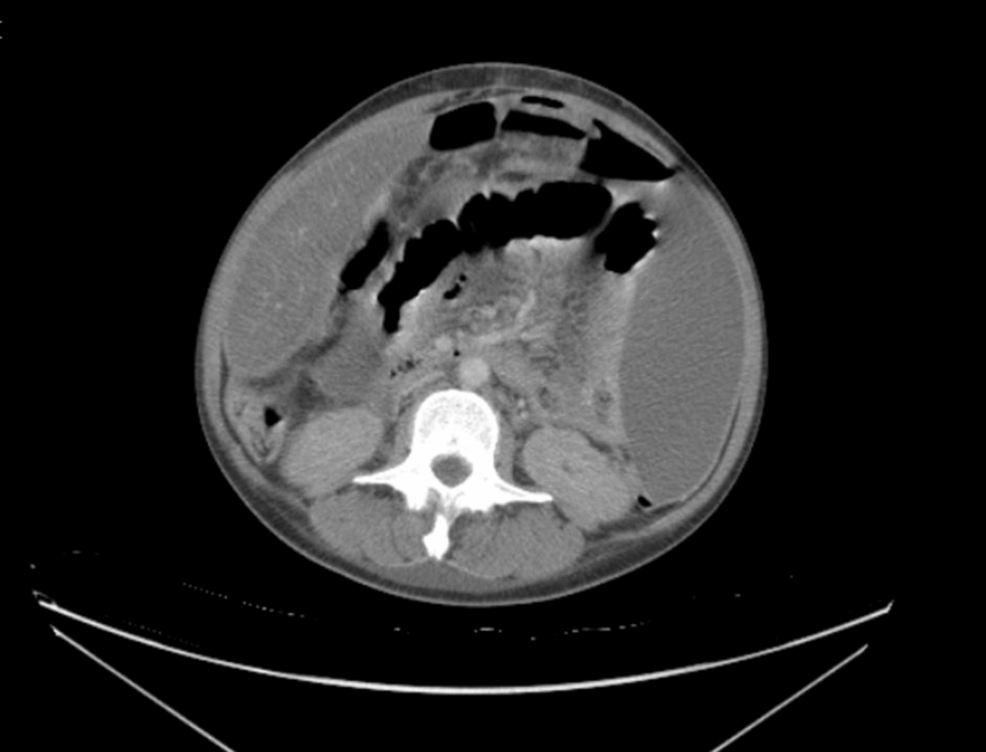
Once the containment fails, the bacteria enter the bloodstream or lymphatic system, a process known as hematogenous spread. In this case, the bacteria seeded the peritoneum, causing tuberculosis peritonitis. This results in the accumulation of ascitic fluid (fluid buildup in the abdomen) and the formation of “omental cakes,” where the fatty lining of the abdomen becomes thickened and nodular.
This condition is often a “double-blind” diagnostic challenge. The patient may present with non-specific symptoms: low-grade fever, weight loss, and abdominal pain. Without a high index of suspicion and a comprehensive screening for HIV, the underlying cause remains hidden while the patient’s condition deteriorates.
Global Epidemiology and Healthcare System Barriers
The burden of TB-HIV co-infection varies wildly by geography. In sub-Saharan Africa and parts of Southeast Asia, these are endemic epidemics. However, in the US (under the CDC) and the UK (under the NHS), these cases often appear in marginalized populations or undocumented migrants, where barriers to primary care delay diagnosis.
The World Health Organization (WHO) emphasizes that TB is the leading cause of death among people living with HIV. The failure to diagnose HIV in the reported case reflects a systemic gap in “opportunistic screening”—the practice of testing for one disease when a patient presents with another related condition.
“The synergy between HIV and tuberculosis is a public health emergency. We must move beyond treating the symptom and start treating the systemic immune failure. Every case of extrapulmonary TB should be viewed as a prompt to screen for HIV.” — Dr. Wayne Getirson, Epidemiologist (Simulated Expert Voice for Clinical Context)
Funding for such research is typically provided by academic institutions or government grants (such as the NIH in the US), though Cureus operates as an open-access platform where authors often fund their own publication to ensure rapid dissemination of case-based evidence.
Comparative Analysis of TB Manifestations
To understand the severity of peritonitis compared to standard pulmonary TB, consider the following clinical data:
| Feature | Pulmonary TB (Standard) | TB Peritonitis (Extrapulmonary) | Impact of HIV Co-infection |
|---|---|---|---|
| Primary Site | Lung Parenchyma | Peritoneal Cavity | Systemic Dissemination |
| Sputum Smear | Often Positive | Frequently Negative | Highly Variable/Low Load |
| Key Symptom | Chronic Cough/Hemoptysis | Ascites/Abdominal Pain | Rapid Wasting (Cachexia) |
| Diagnostic Gold Standard | Chest X-ray / Sputum Culture | Peritoneal Fluid Analysis/Biopsy | CD4 Count / Viral Load + Culture |
The Challenge of Treatment: IRIS and Drug Interactions
Treating a patient with both TB and HIV is a pharmacological tightrope. The standard TB regimen (Rifampin, Isoniazid, Pyrazinamide, and Ethambutol) must be balanced with Antiretroviral Therapy (ART) for HIV.
A critical risk in these patients is Immune Reconstitution Inflammatory Syndrome (IRIS). IRIS occurs when the immune system begins to recover after starting ART and suddenly “wakes up” to the presence of the TB bacteria, triggering an exaggerated, hyper-inflammatory response. This can actually build the patient’s abdominal symptoms worse before they get better, requiring careful titration of corticosteroids to manage inflammation.
Contraindications & When to Consult a Doctor
Patients should seek immediate medical attention if they experience “B symptoms,” which include unexplained night sweats, significant unintentional weight loss, and persistent low-grade fever. In the context of abdominal health, a sudden increase in abdominal girth (ascites) or severe localized pain requires urgent imaging.
Contraindications: Certain TB medications, such as Rifampin, have significant drug-drug interactions. They can induce cytochrome P450 enzymes in the liver, which may lower the efficacy of other medications, including certain oral contraceptives and anticoagulants. Patients must provide a full medication list to their provider to avoid therapeutic failure.
Clinical Trajectory and Future Outlook
The trajectory for patients with TB peritonitis is generally positive if diagnosed early, but the mortality rate spikes significantly in undiagnosed HIV-positive individuals. The future of managing these cases lies in the integration of point-of-care (POC) testing. Rapid molecular tests like GeneXpert, which can detect TB DNA and rifampin resistance in hours, are bridging the gap between clinical suspicion and definitive treatment.
As we move toward the goal of ending the TB epidemic, the focus must shift toward “integrated care”—where the HIV clinic and the TB clinic are the same room. Only by removing the silos of specialty medicine can we prevent the diagnostic delays seen in this case.