
Central nervous system (CNS) fungal infections in Pakistan represent a growing diagnostic challenge, driven by late clinical recognition and the high mortality rates associated with pathogens like Cryptococcus and Aspergillus. Recent synthesis confirms that immunocompromised status and environmental exposure are primary drivers of these life-threatening neurological conditions.
In Plain English: The Clinical Takeaway
- Early Intervention Saves Lives: Fungal infections in the brain often mimic bacterial meningitis; rapid imaging (MRI) and cerebrospinal fluid (CSF) analysis are critical for survival.
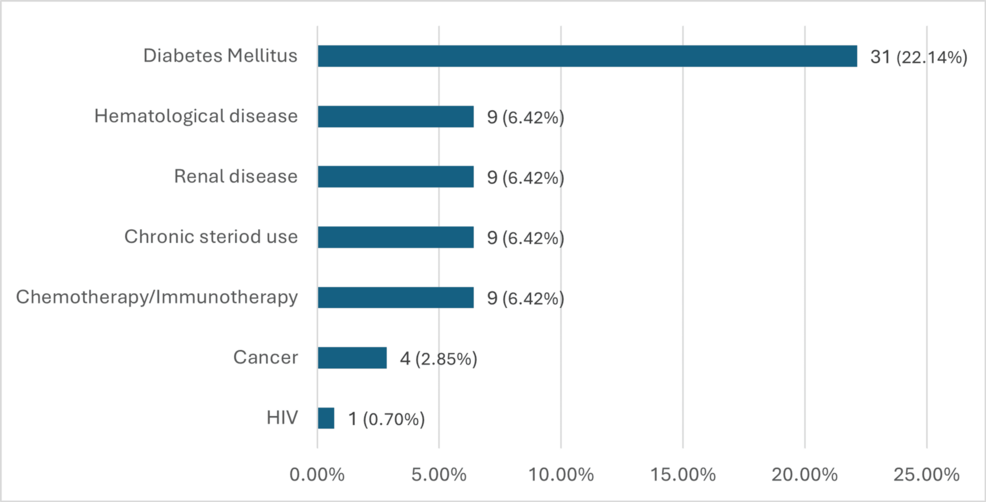
- Risk Awareness: Individuals with diabetes, HIV, or those undergoing long-term corticosteroid therapy face the highest risk of systemic fungal spread to the CNS.
- Treatment Complexity: Antifungal medications, such as amphotericin B and fluconazole, require careful monitoring due to potential kidney toxicity and complex drug-drug interactions.
The Epidemiological Landscape of CNS Fungal Pathogens
The clinical burden of CNS fungal infections in Pakistan is underscored by a lack of standardized diagnostic protocols. According to data published in Cureus, the primary fungal agents identified in regional cohorts include Cryptococcus neoformans, Aspergillus species, and Candida. These organisms typically reach the brain through hematogenous spread—traveling through the bloodstream from a primary site of infection, such as the lungs or sinuses.
.jpg/1280px-Global_Citizen_Festival_Central_Park_New_York_City_from_NYonAir_(15351915006).jpg "In Plain English: The Clinical Takeaway")
The mechanism of action for these infections involves the pathogen breaching the blood-brain barrier (BBB), a highly selective semipermeable border of cells that prevents solutes in the circulating blood from non-selectively crossing into the extracellular fluid of the central nervous system. Once the BBB is compromised, the fungi induce inflammatory responses, leading to cerebral edema (brain swelling), hydrocephalus, or abscess formation.
“The challenge in regions like Pakistan is not just the virulence of the pathogens, but the delay in obtaining definitive microbiological cultures,” notes Dr. Arshad Iqbal, a clinical microbiologist not involved in the original review. “By the time a lumbar puncture confirms a fungal etiology, the neurological damage is often irreversible.”
Comparative Diagnostic and Treatment Outcomes
The following table summarizes the clinical characteristics of the most prevalent fungal pathogens identified in recent regional literature.
| Pathogen | Primary Risk Factor | Standard Treatment | Key Diagnostic Tool |
|---|---|---|---|
| Cryptococcus | HIV/Immunosuppression | Amphotericin B + Flucytosine | CSF India Ink/Antigen Test |
| Aspergillus | Post-surgical/Neutropenia | Voriconazole | MRI Brain / Biopsy |
| Candida | Prolonged ICU Stay | Fluconazole / Echinocandins | Blood/CSF Culture |
Global Health Implications and Resource Allocation
The findings from Pakistan mirror broader concerns voiced by the World Health Organization (WHO) regarding the rising threat of antimicrobial-resistant fungi. In high-income healthcare systems, such as those governed by the NHS in the UK or the FDA in the United States, patients have greater access to rapid molecular diagnostics like PCR-based assays. In contrast, clinicians in resource-limited settings often rely on traditional culture methods, which can take days or weeks to yield results.
Funding for these research initiatives in Pakistan typically stems from institutional grants within medical universities, with limited external pharmaceutical sponsorship. This lack of robust industry funding often results in smaller sample sizes (N-values) in longitudinal studies, making it difficult to establish nationwide incidence rates. Addressing this information gap requires a shift toward centralized surveillance systems that track fungal morbidity in real-time, similar to the CDC’s FungusNET program.
Contraindications & When to Consult a Doctor
Patients currently receiving immunosuppressive therapy, particularly those on prolonged high-dose glucocorticoids or chemotherapy, must maintain a high index of suspicion for neurological changes. Symptoms that necessitate immediate emergency evaluation include:
- Sudden onset of severe, persistent headache.
- Unexplained confusion, lethargy, or altered mental status.
- Focal neurological deficits, such as vision loss, weakness, or slurred speech.
- Nuchal rigidity (stiff neck) accompanied by high fever.
Antifungal treatments are contraindicated in patients with known hypersensitivity to specific classes of azoles or polyenes. Furthermore, clinicians must monitor renal function (creatinine clearance) and electrolyte levels, as systemic antifungal therapy—specifically amphotericin B—is associated with significant nephrotoxicity (kidney damage).
Future Directions in Neuro-Mycology
The narrative review highlights that while our understanding of CNS fungal infections is improving, the clinical trajectory remains poor without early diagnosis. Future efforts must prioritize the deployment of point-of-care diagnostics and the training of neuro-critical care teams in identifying the subtle radiographic signatures of invasive fungal disease. As global travel and climate change alter the distribution of fungal spores, the medical community must treat these infections not as localized anomalies, but as a critical component of infectious disease preparedness.
