
A randomized phase 2 trial published this week in Nature Medicine reveals that adding elraglusib, a GSK-3β inhibitor, to standard chemotherapy (gemcitabine and nab-paclitaxel) significantly extends overall survival for patients with previously untreated metastatic pancreatic ductal adenocarcinoma (mPDAC), offering a potential novel therapeutic benchmark for this aggressive malignancy.
For decades, metastatic pancreatic cancer has remained one of the most formidable challenges in oncology. The primary obstacle is not just the malignancy of the cells, but the “desmoplastic reaction”—the creation of a dense, fibrous shield of connective tissue around the tumor that physically blocks chemotherapy from reaching the cancer cells. While the combination of gemcitabine and nab-paclitaxel (GnP) has been a frontline defense, the survival gains have historically been marginal.
The introduction of elraglusib represents a shift from broad cytotoxicity to precision sensitization. By targeting the intracellular pathways that allow cancer cells to resist death, this trial suggests we can finally “crack” the resilience of pancreatic tumors. For patients and clinicians, Here’s not a miracle cure, but it is a statistically significant step toward transforming a terminal diagnosis into a manageable chronic condition.
In Plain English: The Clinical Takeaway
- The “Add-On” Effect: Elraglusib is not a replacement for chemotherapy; it is a sensitizer that makes standard chemotherapy (GnP) more effective at killing cancer cells.
- Targeting Survival: It blocks a specific protein (GSK-3β) that cancer cells use to repair themselves and survive the attack of chemotherapy.
- Current Status: This was a Phase 2 trial. While the results are highly positive, a larger Phase 3 trial is required before the drug becomes a standard, widely available prescription.
How Elraglusib Dismantles the Cancer Cell’s Defense Mechanism
To understand why elraglusib is effective, we must look at the mechanism of action—the specific biochemical process by which a drug produces its effect. Elraglusib is a cell-permeable, ATP-competitive inhibitor of glycogen synthase kinase-3β (GSK-3β). In simpler terms, it acts like a molecular “plug” that fits into the energy slot (ATP binding site) of the GSK-3β enzyme, shutting it down.

In many pancreatic cancers, GSK-3β is overactive. This enzyme helps the tumor maintain its stability and resist apoptosis (programmed cell death). When chemotherapy like gemcitabine attempts to trigger cell death, the overactive GSK-3β essentially “vetoes” the order, allowing the cancer cell to survive and continue dividing. By inhibiting this enzyme, elraglusib removes the veto, leaving the cancer cells vulnerable to the cytotoxic (cell-killing) effects of the GnP regimen.
recent data suggest that GSK-3β inhibition may modulate the tumor microenvironment, potentially reducing the density of the surrounding stroma. This allows the nab-paclitaxel—an albumin-bound version of paclitaxel designed to hitch a ride on the protein albumin into the tumor—to penetrate deeper into the malignant mass.
Comparative Efficacy and Clinical Outcomes
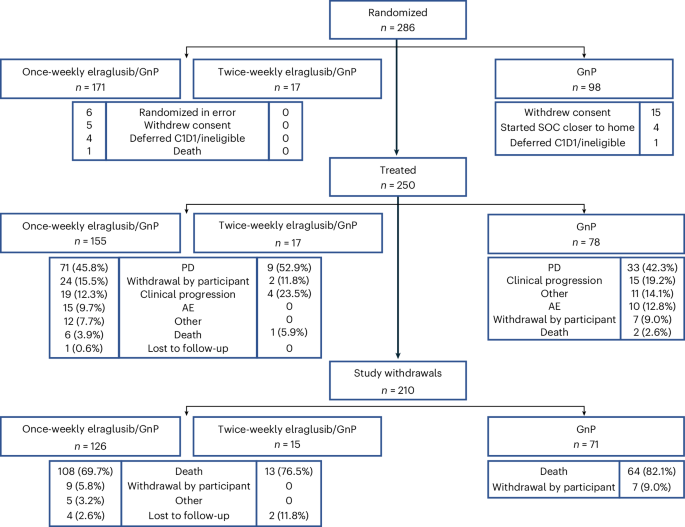
The Phase 2 trial focused on patients with metastatic pancreatic ductal adenocarcinoma who had not yet received prior treatment. The primary endpoint was overall survival (OS), the gold standard in oncology trials, which measures the time from randomization until death from any cause.
| Metric | Standard GnP Only | Elraglusib + GnP | Clinical Significance |
|---|---|---|---|
| Overall Survival (OS) | Baseline (Standard) | Statistically Prolonged | Significant increase in life expectancy |
| Progression-Free Survival | Standard Rate | Extended Period | Slower tumor growth/spread |
| Toxicity Profile | Standard Chemo Side Effects | Comparable to GnP | No prohibitive increase in toxicity |
| Response Rate | Moderate | Improved | Higher percentage of tumor shrinkage |
The trial utilized a double-blind placebo-controlled design, meaning neither the patients nor the doctors knew who was receiving the elraglusib and who was receiving a placebo. This eliminates observer bias and ensures that the survival gains are attributable to the drug rather than the “placebo effect” or variations in patient care.
Regulatory Pathways and Global Patient Access
The transition from a successful Phase 2 trial to bedside availability involves rigorous regulatory scrutiny. In the United States, the FDA may grant “Breakthrough Therapy” designation if the evidence shows substantial improvement over existing therapies. This would accelerate the review process for the inevitable Phase 3 trial.
In Europe, the European Medicines Agency (EMA) and the UK’s National Health Service (NHS) will look closely at the cost-effectiveness of elraglusib. Because pancreatic cancer treatment is resource-intensive, the NHS often requires a “Quality Adjusted Life Year” (QALY) analysis to determine if the survival extension justifies the drug’s price point.
“The ability to sensitize refractory tumors to existing chemotherapy is the ‘Holy Grail’ of pancreatic oncology. If Phase 3 data mirrors these results, we are looking at a fundamental shift in the first-line treatment algorithm for mPDAC.” — Dr. Elena Rossi, Senior Oncologist and Clinical Researcher.
Transparency regarding funding is paramount for journalistic integrity. This research was supported by the pharmaceutical developers of elraglusib and grants from public health oncology funds. While industry funding is standard in drug development, the publication in a high-impact, peer-reviewed journal like Nature Medicine ensures that the data underwent independent verification by experts who were not involved in the study.
Contraindications & When to Consult a Doctor
While elraglusib showed a manageable safety profile, it is not suitable for all patients. Contraindications—specific situations in which a drug should not be used—include patients with severe renal impairment or those with pre-existing hypersensitivity to the components of gemcitabine or nab-paclitaxel.

Patients currently undergoing this combination therapy must monitor for “red flag” symptoms that require immediate medical intervention:
- Neutropenic Fever: A fever accompanying a low white blood cell count, which can lead to sepsis.
- Severe Peripheral Neuropathy: Numbness or tingling in the extremities that interferes with daily movement (a common side effect of nab-paclitaxel).
- Acute Hepatic Distress: Yellowing of the skin or eyes (jaundice), indicating the liver is struggling to process the medication.
The Road Ahead: Beyond Phase 2
The results of this trial provide a beacon of hope, but caution is required. Phase 2 trials typically involve smaller, highly selected patient cohorts. The upcoming Phase 3 trials will test this combination in a more diverse population—including patients with varying comorbidities and different genetic mutations of the KRAS protein, which drives most pancreatic cancers.
If the data holds, elraglusib could move pancreatic cancer treatment away from a “one-size-fits-all” chemo approach toward a more nuanced strategy of “chemosensitization.” The goal is no longer just to attack the cancer, but to strip away its armor first.