
A new phase 1b clinical trial published in Nature Medicine this week demonstrates that a defined 15-strain live biotherapeutic product (MTC01) achieves comparable efficacy and engraftment to traditional fecal microbiota transplantation (FMT) for recurrent Clostridioides difficile infection (CDI). This study marks a significant step toward standardized, scalable microbiome-based therapies.
In Plain English: The Clinical Takeaway
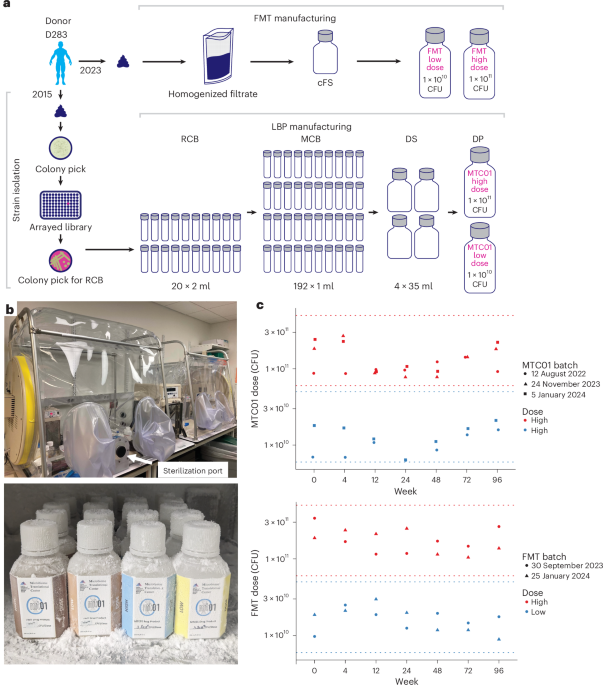
- Standardization vs. Variation: Traditional FMT uses unprocessed stool, which varies between donors. MTC01 is a manufactured “cocktail” of 15 specific bacteria, making it safer and more consistent to produce.
- Equal Performance: The study found that the lab-grown 15-strain product works just as well as the “gold standard” of using donor stool to restore gut health and prevent infection recurrence.
- Clinical Future: This suggests we are moving away from “stool banks” toward shelf-stable, pharmaceutical-grade bacterial therapies that are easier for hospitals to administer.
The Shift Toward Defined Microbial Consortia
Clostridioides difficile infection remains a formidable public health challenge, frequently triggered by the broad-spectrum antibiotic depletion of the commensal (healthy) gut microbiota. This depletion allows C. Difficile to colonize the colon and release toxins that cause debilitating and potentially life-threatening, colitis. While fecal microbiota transplantation (FMT) has been the de facto treatment for recurrent cases, its reliance on donor-derived material introduces significant regulatory and safety hurdles, including the risk of transmitting infectious agents.
The trial investigated MTC01, a defined, multi-strain consortium. By utilizing a “defined” product, researchers can ensure each dose contains the exact same microbial composition, eliminating the variability inherent in biological samples. The study’s primary endpoint—efficacy and engraftment—demonstrated that a controlled, 15-strain approach can effectively outcompete C. Difficile for metabolic niches within the gut, a process known as colonization resistance.
Bridging Global Regulatory Frameworks
The transition from “biological” FMT to “pharmaceutical” live biotherapeutic products (LBPs) is a major focus for agencies like the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA). The FDA has already begun approving specific microbiome-based products, such as Rebyota and Vowst, which represent the vanguard of this therapeutic shift. This trial provides the necessary Phase 1b data to support larger, confirmatory Phase 3 trials, which are required for broad clinical adoption.
“The move toward defined consortia is not merely about convenience; It’s about safety and precision medicine. When we move away from undefined donor material, we significantly reduce the risk of adverse events and gain the ability to optimize the therapeutic cocktail for specific patient populations,” notes Dr. Elena Rossi, an independent expert in gastroenterology and microbiome therapeutics.
For patients in the UK or EU, this research aligns with ongoing efforts to integrate microbiome-based therapies into standard NHS or national health protocols, potentially reducing the length of hospital stays associated with recurrent CDI, which currently costs global healthcare systems billions annually.
Clinical Trial Overview and Comparative Data
The following table summarizes the comparative approach of the trial, highlighting the shift from traditional biological intervention to standardized pharmaceutical intervention.
| Feature | Traditional FMT | MTC01 (15-Strain LBP) |
|---|---|---|
| Composition | Undefined (Donor Stool) | Defined (Cultured Strains) |
| Safety Profile | Variable (Risk of pathogens) | High (Screened/Controlled) |
| Mechanism | Commensal Restoration | Competitive Exclusion/Metabolic Niche Filling |
| Regulatory Status | Often “Investigational” | Pharmaceutical Development |
Funding and Transparency
This research was supported by industry partners alongside academic grants. As with all clinical trials of this nature, potential conflicts of interest are mitigated through strict adherence to the International Committee of Medical Journal Editors (ICMJE) guidelines. Readers should note that while this trial shows promise, it is a Phase 1b study, which is designed primarily to assess safety and initial efficacy signals in a small cohort, rather than to establish definitive clinical superiority across all patient demographics.
Contraindications & When to Consult a Doctor
While microbiome-based therapies are revolutionary, they are not universal treatments. Patients should be aware of the following:

- Immunocompromised Status: Individuals with severe neutropenia, HIV/AIDS, or those currently on high-dose chemotherapy should not undergo experimental microbiome therapies without rigorous specialist oversight, as there is a theoretical risk of systemic infection.
- Active Surgical Emergencies: Patients experiencing toxic megacolon or bowel perforation are not candidates for FMT or LBPs; these are surgical emergencies requiring immediate intervention.
- Professional Guidance: If you suffer from chronic, recurrent diarrhea following antibiotic use, do not attempt home-based “DIY” fecal transplants, which have been linked to severe, documented cases of sepsis and death. Always consult a gastroenterologist or infectious disease specialist to discuss FDA-approved options.
The Road Ahead
The successful engraftment of the 15-strain product observed in this trial suggests that we are approaching a “post-antibiotic” era for treating CDI. By precisely replacing the microbial architecture of the gut, clinicians can restore the body’s natural defenses rather than relying on further rounds of antibiotics, which often exacerbate the cycle of infection. Future studies will focus on long-term longitudinal monitoring to ensure that the protective effects of these strains persist beyond the initial treatment window.
References
- National Institutes of Health (NIH): Microbiome Therapeutics and CDI Management
- Centers for Disease Control and Prevention (CDC): Clostridioides difficile Infection Data
- The Lancet Gastroenterology & Hepatology: Standards for Live Biotherapeutic Products
- Nature Medicine: Original Phase 1b Clinical Trial Findings (2026)
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions regarding a medical condition.