
A 60-year-old man in Spain went to the doctor complaining of a headache that he couldn’t shake. The case was reported in Emerging Infectious Diseases, noting that doctors worked through possible conditions for the patient’s symptoms.
The Diagnostic Pivot: From Malignancy to Parasitology
The patient’s journey began with a two-week progression of worsening headaches and observable behavioral shifts. Initial neurological assessments revealed a mild delay in his movements, but physical examination otherwise remained unremarkable. Because the patient had no history of international travel and was not immunocompromised, the clinical team prioritized metastatic cancer as the primary hypothesis.
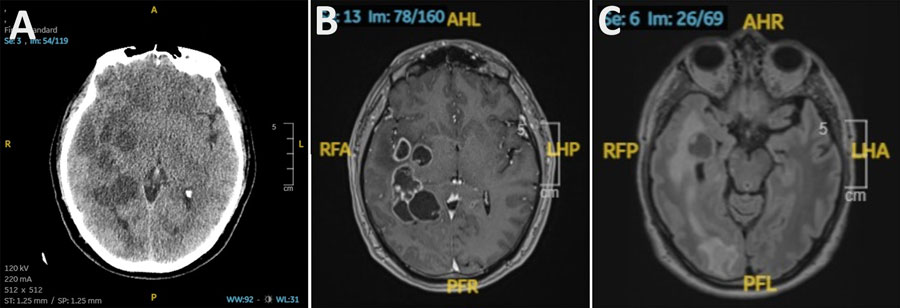
However, the diagnostic focus shifted based on blood work and neuroimaging. While the patient’s systemic markers were largely within reference ranges, his serum Immunoglobulin E (IgE) levels were elevated, a signal of immune responses linked to allergies, autoimmune disease, and parasitic infections. When cross-referenced with the computed tomography (CT) results, which showed multiple lesions distributed throughout his brain accompanied by swelling, the “cancer” hypothesis was challenged.
Decoding the Pathogen
The lesions observed in the patient’s brain were evidence of a problem. The “behavioral changes” reported by the patient were noted by the doctors.
The difficulty in diagnosis stems from the radiological overlap between conditions. In a case report, the doctors reported working through the possible conditions that could explain all the findings.
The Data Gap
The patient’s lack of international travel history is a critical data point. The doctors noted that the man had never traveled internationally.
Managing Neuro-Inflammatory Response
The treatment protocol for this patient required a departure from oncological surgical intervention. Instead, the team utilized a combination of anti-parasitic agents and corticosteroids to manage the intracranial swelling. Managing the inflammatory response is essential; as the parasites die, they release antigens that can trigger a massive immune surge, further increasing cerebral edema.
- Primary Diagnostic Signal: Elevated IgE levels in the blood.
- Imaging Artifacts: Multiple lesions accompanied by swelling.
- Clinical Key: Behavioral changes and mild delay in movements.
The 30-Second Verdict: Lessons for Modern Diagnostics
This case underscores the limitations of relying on heuristic diagnostic models—or “clinical intuition”—that prioritize common conditions like cancer while overlooking rare infectious entities. In an era of advanced medical imaging, the human element of interpreting those images remains the ultimate point of failure. The report serves as a reminder that even in patients without travel history, the “zebra” in the room might be a parasite.
For clinicians, the takeaway is clear: when neuroimaging reveals multiple lesions, the differential diagnosis must include parasitic infections even if the patient appears to be a low-risk candidate. Accurate testing for parasitic antibodies and careful consideration of immune markers like IgE are not just supplementary; they are critical verification steps that prevent unnecessary, invasive, and potentially harmful oncological treatments.