
{kind=link}
Medicaid Payment Shake-Up: States Face Potential Cuts Under New Bill
Table of Contents
- 1. Medicaid Payment Shake-Up: States Face Potential Cuts Under New Bill
- 2. Bill’s Impact on State-Directed Payments
- 3. States Facing Potential Payment Reductions
- 4. Understanding State-Directed Payments (SDPs)
- 5. Benchmark Practices Among States
- 6. The Role of Commercial Rates in Ensuring Adequate Provider Networks
- 7. Potential Impact of Provider Tax Changes
- 8. Summary of Potential Impact on States
- 9. Evergreen insights on Medicaid Funding
- 10. Frequently Asked Questions
- 11. Here are some PAA-related questions based on the provided context and the available search results:
- 12. Medicaid Cuts Loom for Hospitals and nursing Facilities: Navigating the Reconciliation Landscape
- 13. Understanding the Implications of Medicaid Cuts
- 14. Direct Financial Impacts
- 15. Patient Access and Quality of Care Concerns
- 16. Strategies for Hospitals and Nursing Facilities
- 17. Financial Planning and Operational Efficiency
- 18. Exploring Alternative Revenue Streams
- 19. advocacy and Policy Engagement
- 20. Real-World Examples and Case Studies
A New Congressional Bill could trigger considerable changes in how states fund healthcare, especially impacting hospitals and nursing facilities through Medicaid. The proposed legislation aims to curb federal Medicaid spending, potentially forcing nearly 30 states to adjust their payment structures.
Bill’s Impact on State-Directed Payments
The “One Big Beautiful Bill Act,” previously passed by the House, seeks to reduce federal Medicaid spending significantly over the next decade. A key component of this act targets state-directed payments (SDPs), which enable states to guide how managed care organizations (MCOs) compensate healthcare providers. These payments frequently enough aim to boost provider payment rates, enhancing both access to and the quality of care.
Under the proposed changes, future SDPs for hospitals and nursing facilities would be capped at 100% of Medicare rates in states that have expanded Medicaid and 110% in non-expansion states.Moreover, a draft reconciliation language from the Senate Finance Committee suggests a further reduction of existing SDPs by 10% annually until they align with these statutory limits.
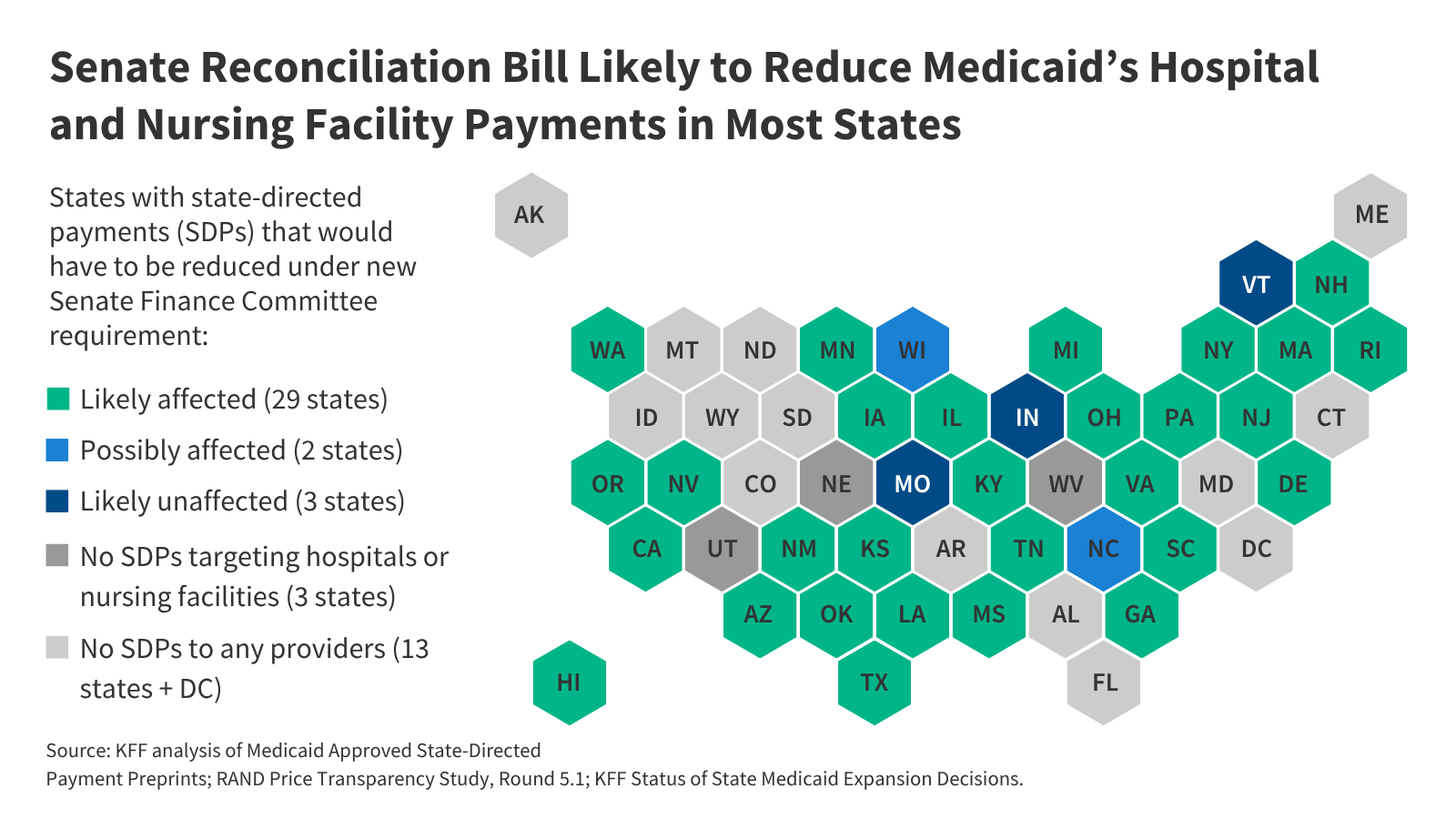
States Facing Potential Payment Reductions
An analysis reveals that if the bill passes with the Finance Committee’s SDP requirements, approximately 29 states would likely experience decreased payments to hospitals or nursing facilities. This number could potentially rise above 31 states. The review scrutinized SDP arrangements approved by the Centers For Medicare & Medicaid Services (CMS).
While the primary focus remains on payments to hospitals and nursing facilities, other provider payments could also be affected, especially in SDPs that cover multiple provider types with varying payment limits.
Did You Know? SDPs are a critical tool states use to manage and improve healthcare delivery within their Medicaid programs. These payments can significantly influence provider participation and service quality.
Understanding State-Directed Payments (SDPs)
Managed care is the predominant model for Medicaid beneficiaries, with 75% enrolled in comprehensive MCOs across 42 states. SDPs offer states a mechanism to direct MCO payments under specific conditions, such as setting minimum or maximum fee schedules, providing uniform payment increases, implementing value-based purchasing models, or participating in delivery system reform initiatives.
These actions are governed by federal regulations (42 CFR 438.6(C)), requiring states to obtain CMS approval before implementing SDPs, unless the SDP uses a minimum fee schedule equivalent to Medicare or Medicaid fee-for-service rates.
Pro Tip: States can leverage SDPs to address specific healthcare needs within their populations,such as improving access to specialized care or incentivizing better health outcomes through value-based payment models.
Benchmark Practices Among States
Most states with SDPs for hospitals or nursing facilities benchmark at least one state-directed payment against average commercial rates. These benchmarks, documented in pre-approval submissions to CMS, help establish payment levels required of MCOs.
Notably, 24 states have at least one SDP that raises reimbursement to over 90% of average commercial rates. In contrast, fewer states benchmark against Medicare or Medicaid fee-for-service rates.
Reader Engagement question #1: How do you think these potential medicaid payment changes will affect access to healthcare services in your state?
The Role of Commercial Rates in Ensuring Adequate Provider Networks
The practice of tying payments to average commercial rates was intended to secure adequate provider networks and encourage the adoption of value-based payment methods. A 2024 rule on Medicaid managed care formalized this approach, setting the maximum payment rate for hospital services, nursing facility services, and qualified practitioner services at academic medical facilities at the average commercial payment rate (ACR).
Potential Impact of Provider Tax Changes
Moreover, the bill under consideration could potentially require 22 states to cut provider taxes on hospitals or managed care organizations, which would exacerbate the effects of cutting existing SDPs for the states that are jointly affected. Because provider taxes often fund SDPs, even states with SDPs below permissible levels could be forced to cut their provider payment rates if they are affected by the lower provider tax thresholds.
Reader Engagement Question #2: What strategies could states use to mitigate the potential negative impacts of these Medicaid payment changes on healthcare providers and patients?
Summary of Potential Impact on States
here’s what the proposed changes could mean for states:
| Category | Description |
|---|---|
| States Likely Affected | Approximately 29 states may see decreased payments to hospitals and nursing facilities. |
| Payment Benchmarks | Many states benchmark SDPs against average commercial rates, potentially exceeding proposed caps. |
| Policy Goal | Aims to reduce federal Medicaid spending and standardize payment rates. |
Evergreen insights on Medicaid Funding
Changes in Medicaid funding models can have long-lasting effects on state budgets and healthcare delivery systems. States frequently enough need to develop innovative strategies to maintain service levels while adapting to new fiscal realities.
Considerations for states include:
- CMS Guidance: Staying informed about federal guidelines and waivers can help states maximize available funding and adaptability.
-
Value-Based Care: Transitioning to payment models that reward quality and outcomes can improve efficiency and reduce costs.
-
Provider Collaboration: Engaging with healthcare providers to find mutually beneficial solutions can ease the transition to new payment structures.
Frequently Asked Questions
-
What are state-directed payments (SDPs) in Medicaid?
State-directed payments (SDPs) are mechanisms that allow states to direct how Medicaid managed care organizations (MCOs) pay healthcare providers, often to boost payment rates and improve access to care. -
How might the proposed bill affect existing Medicaid SDPs?
The proposed bill could reduce existing SDPs by 10% each year until they align with new statutory limits, potentially impacting numerous states. -
Which states are most likely to be affected by these Medicaid payment changes?
Approximately 29 states could see required payments to hospitals or nursing facilities decrease, with potentially more than 31 states affected. -
What benchmarks do states typically use for SDPs?
Many states use average commercial rates to benchmark their state-directed payments, though some also use Medicare or Medicaid fee-for-service rates. -
Why were SDPs tied to average commercial rates?
Tying payments to average commercial rates was intended to ensure adequate provider networks and promote the use of value-based payment methods.
How do you feel about these potential changes? Share your thoughts and comments below.
The healthcare landscape is constantly evolving, and recent discussions surrounding potential Medicaid cuts through the reconciliation process have created significant concerns for hospitals and nursing facilities. These cuts could have far-reaching consequences, impacting financial stability, access to care, and the overall quality of services provided to vulnerable populations. Understanding the potential ramifications and proactive strategies is crucial for these healthcare providers to navigate the challenges ahead.
Understanding the Implications of Medicaid Cuts
Medicaid, a joint federal and state program, represents a significant source of revenue for many hospitals and nursing homes. Cuts to Medicaid reimbursement rates, or reductions in eligibility, directly impact the financial health of these facilities. This section delves into the specific areas likely to be affected by these potential cuts, including financial impacts, decreased patient access to care, and potential impacts on staffing.
Direct Financial Impacts
- Reduced Reimbursement Rates: Lower payments for services provided to Medicaid patients.
- Decreased Revenue: Potential loss of millions of dollars in revenue,especially for facilities with a high percentage of Medicaid patients.
- Budgetary Constraints: Difficulties in covering operational costs, including staffing, supplies, and infrastructure.
- Impact on Hospital Capacity: Hospitals may have to reduce beds or services to maintain financial viability.
Patient Access and Quality of Care Concerns
Medicaid cuts can negatively affect a patient’s healthcare access and can result in the following:
- Reduced Access to Care: potential reductions in access to care for Medicaid beneficiaries.
- Service Limitations: Potential cuts to essential services such as long-term care, rehabilitative services, and behavioral health.
- Quality of Care Concerns: Possibility of less focus on quality of care if financial resources are more limited.
- Nursing Home challenges: Nursing homes may struggle with adequate staffing levels impacting the quality of care.
Strategies for Hospitals and Nursing Facilities
Healthcare providers can take steps to mitigate the adverse effects of Medicaid cuts. These strategies require careful planning, resourcefulness, and a focus on efficiency. these include financial planning, exploring alternative revenue streams, and advocating for policy changes.
Financial Planning and Operational Efficiency
- Detailed Budgeting: Develop detailed budgets projecting potential revenue shortfalls.
- Cost Containment: Focus on reducing costs through process optimization and vendor negotiation.
- Efficient Resource Allocation: Strategic allocation of resources to prioritize essential services.
- Operational optimization: Improve workflows and reduce waste to enhance efficiency.
Exploring Alternative Revenue Streams
Diversifying revenue sources can provide a financial cushion against Medicaid cuts.
- Expand Private Pay Options: Attract patients with private insurance or the ability to pay directly.
- Seek Grants and Funding: Explore grant opportunities to support specific programs.
- Develop New Services: Offer new services that generate additional revenue.
- Improve Revenue Cycle Management: ensure accurate billing and timely collections.
advocacy and Policy Engagement
Healthcare providers should engage in advocacy to shape policy decisions positively.
- Lobbying Efforts: Advocate for policies that protect Medicaid funding and reimbursement rates.
- Community Engagement: raise awareness about the impact of cuts on patients and the community.
- Collaboration: work with other healthcare providers and industry associations.
- Public awareness: Educate the public about the essential role of Medicaid and potential impact of cuts.
Real-World Examples and Case Studies
Understanding how these challenges affect providers, and what solutions they pursue can provide significant context.
case Study: A rural hospital experienced a 15% reduction in Medicaid reimbursements, leading to cuts in staffing and a reduction in outpatient services. The hospital then focused on process improvements and pursued grant funding. Eventually, they secured funding for a telehealth program, which provided better patient access and improved financial sustainability.
Example: A nursing home, facing Medicaid cuts, expanded its private pay options and enhanced its marketing efforts. They improved their patient care services. The nursing home successfully increased occupancy rates. They improved their profit and maintained a high level of care.
| Challenge | Strategy | Outcome |
|---|---|---|
| Reduced Medicaid Reimbursement | Cost-Cutting & Process Improvements | Maintained Financial Stability & Prevented Service Reductions |
| Decreased Patient Volume | Focus on Higher Quality of Patient Care | Increased Patient Satisfaction and Referral Rates. |
| inadequate Staffing Levels | Employee Retention Program | Reduced staff turnover and ensured appropriate staffing levels |