
State Medicaid agencies are finalizing spending reports on State Directed Payments (SDPs) ahead of federal regulatory changes mandated by recent reconciliation legislation. These payments, which allow states to direct how managed care organizations pay providers, face new oversight thresholds designed to improve fiscal transparency and ensure clinical accountability in public health.
In Plain English: The Clinical Takeaway
- Fiscal Oversight: New federal rules will require states to provide more granular data on how supplemental payments to hospitals and clinics actually improve patient outcomes.
- Access Stability: These payments are often used to bridge funding gaps for safety-net hospitals; changes in policy may influence the availability of specialized care in underserved regions.
- Clinical Outcomes: The shift aims to move Medicaid funding away from general “pass-through” payments toward models that reward specific, measurable health metrics like reduced readmission rates.
The Mechanism of State Directed Payments
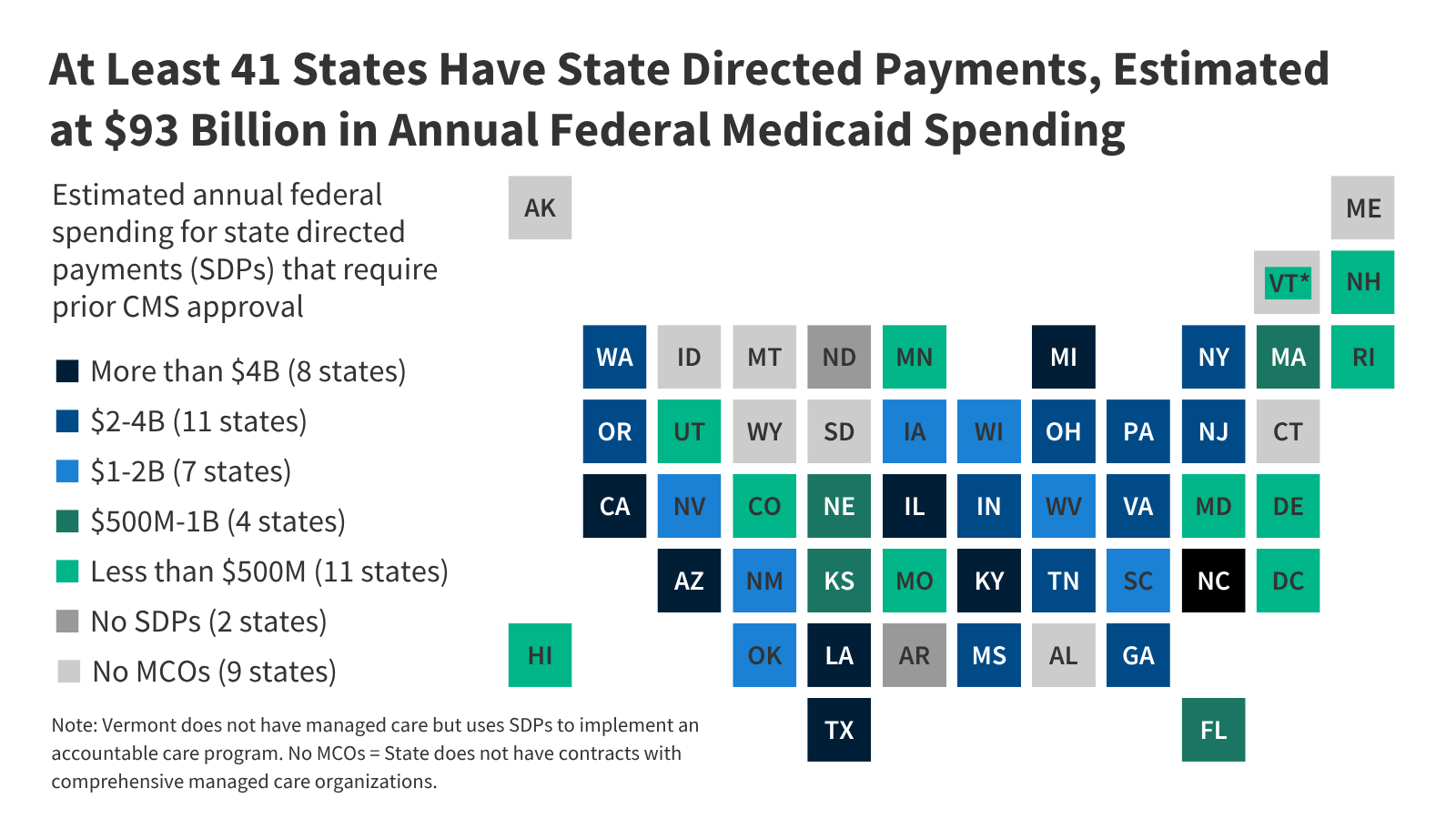
State Directed Payments (SDPs) serve as a financial lever within Medicaid managed care. Under these arrangements, states require managed care plans to pay providers specific amounts, often to bolster funding for public hospitals or to incentivize participation in value-based care initiatives. According to the Centers for Medicare & Medicaid Services (CMS), these payments must be grounded in a written approval process that demonstrates the payment structure is consistent with the access and quality standards of the underlying managed care contract.
The reconciliation law, which introduced stricter reporting and approval requirements, seeks to curb the use of supplemental payments that lack direct links to clinical performance. By requiring states to demonstrate that SDPs are “budget neutral” or tied to specific quality benchmarks, federal regulators aim to prevent the inflation of administrative costs without corresponding improvements in patient care delivery.
“The transition toward value-based purchasing in Medicaid is not merely a bureaucratic shift; it is a fundamental change in how we define the value of a healthcare dollar. We must ensure that every public subsidy is tethered to a verifiable clinical endpoint,” noted Dr. Elena Rodriguez, a senior health policy analyst at the Kaiser Family Foundation.
Geo-Epidemiological Impact on Patient Access
The impact of these financial shifts varies significantly by state, particularly in regions with a high density of rural safety-net hospitals. In states where SDPs have historically accounted for a large portion of hospital revenue, the new federal limits may force a restructuring of how those facilities deliver care. Epidemiological data suggests that rural populations rely disproportionately on these facilities for chronic disease management, including the treatment of diabetes and hypertension.
When funding streams are disrupted or restricted, the risk of “care deserts”—geographic areas lacking essential medical services—increases. Data from the CDC’s Office of Rural Health indicates that financial instability in local hospital systems is a primary driver of delayed screenings and poor management of acute conditions in rural cohorts. The current regulatory tightening forces states to justify these payments through the lens of clinical necessity rather than just institutional solvency.
| Metric | Pre-Regulation Status | Post-Regulation Requirement |
|---|---|---|
| Approval Standard | General programmatic oversight | Evidence-based clinical performance |
| Transparency | Aggregated state-level reporting | Provider-specific impact analysis |
| Primary Goal | Institutional financial support | Patient outcome optimization |
Funding and Bias Transparency
The analysis of these fiscal shifts is informed by public records and budget briefs provided by the Medicaid and CHIP Payment and Access Commission (MACPAC). MACPAC is a non-partisan legislative branch agency that provides policy and data analysis to Congress. This reporting relies on their independent assessment of state-submitted data. No external pharmaceutical or private insurance interests have influenced the analysis of these regulatory changes, maintaining the integrity of the information provided to the public.

Contraindications & When to Consult a Doctor
While these policy shifts do not directly alter clinical treatments, patients who rely on Medicaid for specialized care should be aware of potential changes in their network coverage. If a local facility undergoes a change in funding model, patients may experience shifts in the availability of specific outpatient services or referrals. Consult your primary care physician or a patient navigator if you notice unexpected changes in your insurance coverage or the closure of specific clinic departments. Always verify that your provider remains in-network with your Medicaid managed care plan before scheduling elective procedures to avoid unforeseen out-of-pocket costs.
Future Trajectory of Medicaid Financing
As the new limits take effect, the focus of federal oversight will likely shift toward longitudinal studies of patient outcomes. The goal is to determine whether the redirection of funds toward specific performance metrics results in a measurable decrease in morbidity or an improvement in population health statistics. By prioritizing clinical efficacy over blanket subsidies, the federal government is attempting to modernize Medicaid to better serve the evolving needs of the millions of individuals who rely on the program for essential medical services.
References
- Centers for Medicare & Medicaid Services (CMS): State Directed Payments Guidance
- Medicaid and CHIP Payment and Access Commission (MACPAC): Analysis of Managed Care SDPs
- Centers for Disease Control and Prevention (CDC): Rural Health and Access to Care
Disclaimer: This article is for informational purposes only and does not constitute medical, legal, or financial advice. Always consult with a qualified healthcare provider or official state Medicaid resources regarding specific coverage questions.