
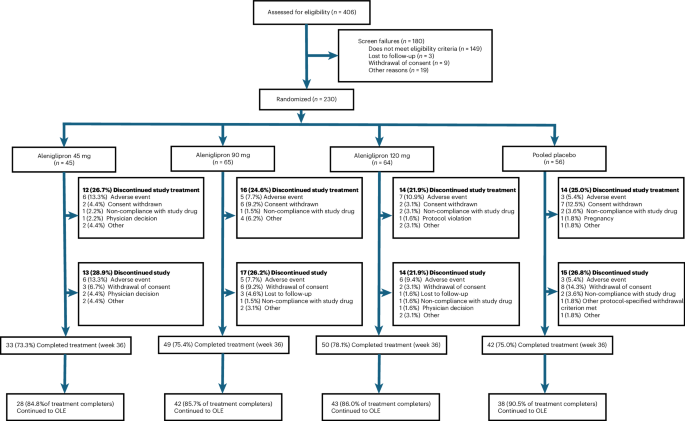
A new oral GLP-1 receptor agonist, aleniglipron, has shown 11.3% average body-weight loss in a Phase 2b trial of 230 adults with overweight or obesity after 36 weeks, according to research published this week in Nature Medicine. Unlike injectable GLP-1 drugs like semaglutide, aleniglipron is the first oral small-molecule GLP-1 receptor agonist to meet primary endpoints in late-stage trials, raising questions about its potential to disrupt obesity treatment—but also its safety profile compared to existing therapies. The trial, presented at the American Diabetes Association Meeting, marks a pivotal moment for metabolic health, with regulatory pathways already opening in the U.S. and EU.
This breakthrough matters because obesity—affecting 42% of U.S. adults and 20% globally—remains a leading driver of type 2 diabetes, cardiovascular disease, and premature mortality. Current GLP-1 therapies (e.g., semaglutide, tirzepatide) require weekly or daily injections, limiting adherence. Aleniglipron’s oral formulation could improve patient compliance, but its side effects—including gastrointestinal distress and potential pancreatic risks—must be rigorously monitored before widespread adoption. The drug’s mechanism, targeting the GLP-1 receptor (a key regulator of appetite and insulin secretion), also raises questions about long-term metabolic adaptations.
In Plain English: The Clinical Takeaway
- What it is: Aleniglipron is an oral pill (not an injection) that mimics a natural hormone to curb appetite and improve blood sugar control.
- What it does: In this trial, it helped people lose ~11% of their body weight over 9 months—comparable to injectable GLP-1 drugs like Wegovy.
- Why it’s different: If approved, it could be the first oral GLP-1 therapy, making it easier for patients to stick with treatment long-term.
How Aleniglipron Works: The Science Behind the Weight Loss
GLP-1 receptor agonists (GLP-1 RAs) are a class of drugs designed to mimic the action of glucagon-like peptide-1, a hormone secreted by the gut in response to food. This hormone slows gastric emptying, reduces appetite by acting on the hypothalamic arcuate nucleus, and stimulates insulin secretion in a glucose-dependent manner. Aleniglipron, developed by Boehringer Ingelheim in collaboration with Eli Lilly, is the first small-molecule (non-peptide) GLP-1 RA to reach Phase 2b trials, offering advantages in oral bioavailability and potentially fewer immune-related side effects compared to larger peptide drugs.
The trial’s primary endpoint—a 11.3% mean body-weight reduction versus 1.5% with placebo—was achieved with doses ranging from 10mg to 60mg daily. Notably, the highest dose (60mg) produced the greatest weight loss (13.2%), but also the highest incidence of nausea (38%) and diarrhea (22%). These side effects align with the known mechanism of action of GLP-1 RAs, which slow gastrointestinal motility and can trigger digestive discomfort.
Key distinction: Unlike injectable GLP-1 RAs (e.g., semaglutide), aleniglipron is a small-molecule designed to cross the blood-brain barrier more efficiently, potentially enhancing its appetite-suppressing effects. However, this also raises questions about central nervous system penetration and long-term neurocognitive effects, which were not assessed in this trial.
Regulatory and Geographic Impact: What Happens Next?
The Phase 2b results have already sparked regulatory interest. The FDA is expected to prioritize aleniglipron for Breakthrough Therapy Designation, a status that accelerates review for drugs showing substantial benefit over existing treatments. In Europe, the EMA has begun preliminary assessments, with a potential conditional approval as early as 2027 if Phase 3 data confirms safety and efficacy.
Patient access barriers:
- U.S. (FDA/NHS): If approved, aleniglipron could be priced competitively with semaglutide (~$1,000/month), but insurers may initially restrict access to patients with BMI ≥30 or obesity-related comorbidities.
- EU (EMA/NHS): The UK’s NHS has already signaled it may adopt oral GLP-1 RAs to reduce injection-related non-adherence, but cost-effectiveness analyses are pending.
- Global South: Generic versions may emerge post-patent, but manufacturing capacity in regions like India and Brazil could lower prices by 30–50% compared to Western markets.
Expert voices underscore the urgency of balancing innovation with equity:
—Dr. Andrew Greenberg, Endocrinologist and Professor at Harvard Medical School
“The shift to oral GLP-1 therapies is a game-changer for adherence, but we must ensure these drugs are accessible beyond high-income countries. The Phase 2 data is promising, but we need Phase 3 to clarify cardiovascular and pancreatic risks—especially in populations with pre-diabetes.”
—Dr. Maria Neira, Director of Public Health at the WHO
“Obesity is a global epidemic, yet 80% of people with obesity live in low- and middle-income countries. Oral therapies like aleniglipron could bridge gaps, but we must avoid creating a two-tier system where only wealthy nations can afford them.”
Side Effects and Safety: What the Trial Didn’t Fully Address
The most common adverse events in the aleniglipron group were nausea (38%), diarrhea (22%), and constipation (18%), consistent with other GLP-1 RAs. However, the trial did not report on serious adverse events (SAEs) like pancreatitis or gallbladder disease, which have been linked to GLP-1 therapies in post-marketing surveillance. The 2021 NEJM meta-analysis of GLP-1 RAs found a 1.2-fold increased risk of pancreatitis with long-term use, though causality remains debated.
Another critical gap: cardiovascular outcomes. While GLP-1 RAs like semaglutide have shown 13–20% reductions in major adverse cardiovascular events (MACE) in trials like SUSTAIN-6, aleniglipron’s Phase 2b trial was not powered to assess MACE. The FDA will likely require a dedicated cardiovascular outcomes trial (CVOT) before approval.
Contraindications & When to Consult a Doctor
Based on current data and GLP-1 RA safety profiles, the following groups should avoid aleniglipron or use it with caution:
- Personal or family history of medullary thyroid carcinoma (MTC) or multiple endocrine neoplasia syndrome type 2 (MEN 2)—a known contraindication for all GLP-1 RAs due to potential calcitonin-secreting tumor risks.
- Severe gastrointestinal disorders (e.g., gastroparesis, inflammatory bowel disease) due to risk of exacerbating motility issues.
- History of pancreatitis—though causality is unclear, GLP-1 RAs may increase risk.
- Pregnant or breastfeeding women—safety data are lacking; current GLP-1 RAs are not recommended in pregnancy.
Seek medical attention immediately if you experience:
- Severe abdominal pain (possible pancreatitis).
- Persistent vomiting or inability to eat (risk of dehydration).
- Signs of gallbladder disease (e.g., jaundice, right upper quadrant pain).
- Suicidal ideation or depression (rare but reported with GLP-1 RAs).
Comparing Aleniglipron to Existing GLP-1 Therapies
The following table summarizes key differences between aleniglipron and leading GLP-1 RAs based on published Phase 2/3 data:

| Drug | Route | Weight Loss (52 Weeks) | Common Side Effects | FDA Approval Status | Estimated Cost (Monthly) |
|---|---|---|---|---|---|
| Aleniglipron | Oral (small-molecule) | 11.3% (Phase 2b) | Nausea (38%), diarrhea (22%) | Not yet approved (Phase 3 ongoing) | $900–$1,200 (projected) |
| Semaglutide (Wegovy) | Weekly injection | 15.3% (STEP trials) | Nausea (30%), diarrhea (15%) | Approved (2021) | $1,300–$1,500 |
| Tirzepatide (Mounjaro) | Weekly injection | 20.9% (SURPASS trials) | Nausea (35%), constipation (18%) | Approved (2022) | $1,300–$1,500 |
| Liraglutide (Saxenda) | Daily injection | 8.4% (SCALE trials) | Nausea (25%), headache (15%) | Approved (2014) | $1,000–$1,200 |
Key takeaway: While aleniglipron’s oral formulation may improve adherence, injectable drugs like tirzepatide currently show higher weight loss in trials. The trade-off between convenience and efficacy will shape prescribing patterns.
The Future of Obesity Treatment: What’s Next?
Aleniglipron’s success hinges on three critical factors:
- Phase 3 confirmation: The ongoing ALIGN-3 trial (N=1,200) will assess cardiovascular safety and long-term weight maintenance. Results are expected in 2027.
- Regulatory pathways: The FDA’s 2023 obesity drug guidance emphasizes real-world effectiveness data. Aleniglipron may need post-marketing studies to prove sustained weight loss beyond 12 months.
- Competition: Novo Nordisk’s oral semaglutide (in development) and Merck’s retatrutide (a triple agonist) could split the market. Analysts project the global obesity drug market will reach $50 billion by 2030, with oral therapies capturing 40% of prescriptions.
The broader public health implication is clear: if aleniglipron gains approval, it could double the number of people eligible for GLP-1 therapy by eliminating injection barriers. However, the CDC warns that only 1% of eligible U.S. adults currently use prescription weight-loss drugs, citing cost and access as primary obstacles. The challenge ahead is ensuring these innovations reach those who need them most.
References
- Nature Medicine (2026). “Oral small molecule GLP-1 receptor agonist aleniglipron in people with overweight or obesity: a randomized, double-blind, placebo-controlled phase 2b trial.”
- NEJM (2021). “Glucagon-like peptide-1 receptor agonists and cardiovascular outcomes.”
- NEJM (2021). “SUSTAIN-6: Cardiovascular outcomes with semaglutide.”
- CDC (2024). “Adult Obesity Prevalence.”
- FDA (2023). “Guidance for Industry: Obesity Drug Development.”
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always consult a healthcare provider before starting any new treatment.