
Following new research published this week, pediatric cardiologists are advocating for a revised approach to newborn screening that incorporates pulse oximetry testing earlier and more universally to detect critical congenital heart disease (CCHD), a group of structural heart defects present at birth that can lead to life-threatening complications if undiagnosed. The proposal, informed by multicenter data from the U.S. And Europe, aims to close persistent gaps in detection rates, particularly among infants born outside hospital settings or in under-resourced clinics, where current screening protocols show inconsistent implementation. By lowering the threshold for intervention and standardizing follow-up echocardiograms, experts estimate that up to 30% more cases of CCHD could be identified before hospital discharge, significantly improving surgical outcomes and reducing neonatal mortality.
In Plain English: The Clinical Takeaway
- Critical congenital heart disease affects about 2 in every 1,000 newborns and can cause severe oxygen deprivation if not caught early.
- A simple, non-invasive test called pulse oximetry—measuring oxygen levels in the blood via a sensor on the hand or foot—can detect most cases before symptoms appear.
- Experts now recommend performing this test universally within 24 to 48 hours of birth, followed by immediate echocardiogram if results are abnormal, to ensure timely surgical planning.
Why Current Newborn Screening Misses Critical Heart Defects
Despite the 2011 endorsement by the U.S. Secretary of Health and Human Services for universal pulse oximetry screening, implementation remains fragmented across states and birthing facilities. A 2023 CDC analysis revealed that nearly 15% of U.S. Birth centers still do not routinely perform the test, with the lowest compliance rates observed in home births and rural clinics lacking trained personnel or access to echocardiography for confirmation. Internationally, the picture is similarly uneven: while countries like the UK and Sweden have achieved near-universal screening through national health service mandates, many low- and middle-income nations lack both the infrastructure and funding to scale such programs. This variability contributes to delayed diagnosis, with studies showing that up to 40% of infants with CCHD are discharged before their defect is detected, increasing the risk of circulatory collapse and neurological injury.

The Science Behind Pulse Oximetry in CCHD Detection
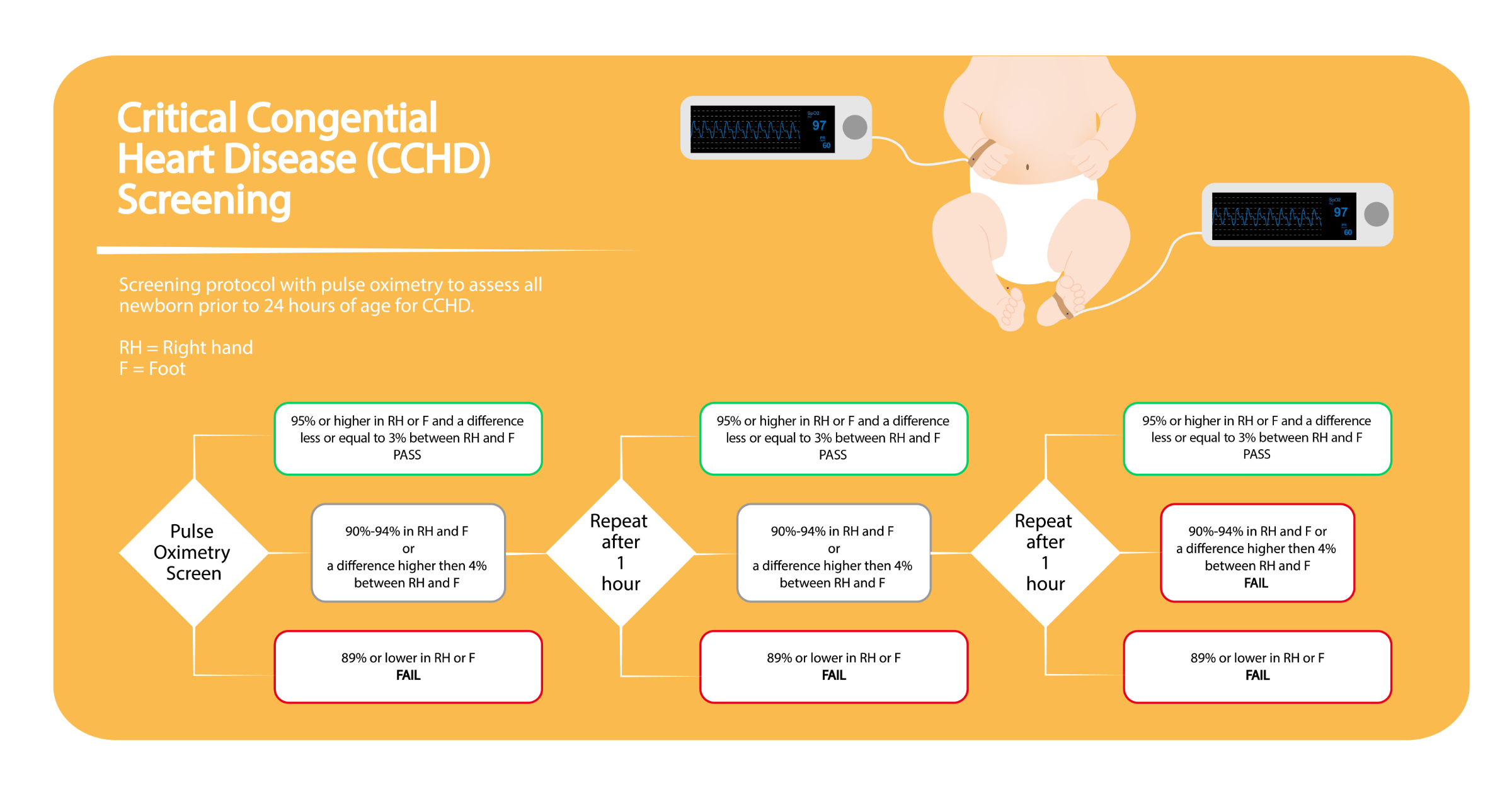
Pulse oximetry works by measuring the saturation of hemoglobin with oxygen in peripheral blood, typically via a light-emitting sensor placed on the skin. In newborns with certain forms of CCHD—such as hypoplastic left heart syndrome, pulmonary atresia, or tetralogy of Fallot—abnormal blood flow patterns reduce oxygen delivery to the body, resulting in lower-than-normal arterial oxygen saturation (SpO₂). While healthy newborns typically maintain SpO₂ levels above 95%, infants with CCHD often register readings below 90% in one or more extremities. The screening protocol, endorsed by the American Academy of Pediatrics, involves measuring oxygen saturation in the right hand and either foot; a difference of more than 3% between sites or a reading below 90% in either limb triggers a positive screen, necessitating immediate diagnostic echocardiography.

“Pulse oximetry doesn’t diagnose the specific heart defect, but it acts as a powerful physiological stress test—identifying when a newborn’s circulation is unable to meet metabolic demands, which is often the first detectable sign of critical disease.”
— Dr. Catherine Zahn, Director of Fetal Cardiology, Boston Children’s Hospital, and lead author of the 2024 multicenter validation study published in Circulation.
Global Implementation and Health System Integration
In the United States, the Centers for Disease Control and Prevention (CDC) continues to monitor state-level adherence through the National Birth Defects Prevention Network, with recent data showing that states mandating pulse oximetry by law—such as California, New York, and Texas—have seen a 22% reduction in late detection of CCHD compared to states with only voluntary guidelines. The Food and Drug Administration (FDA) has cleared multiple pulse oximetry devices specifically for neonatal use, though it does not regulate screening protocols, leaving enforcement to state health departments. In Europe, the European Medicines Agency (EMA) does not oversee screening tools, but the European Society of Cardiology recommends universal pulse oximetry as part of the Newborn and Infant Physical Examination (NIPE) program, which is integrated into postnatal care pathways in the UK’s National Health Service (NHS) and similar systems in Germany and the Netherlands. In contrast, nations without centralized newborn health registries, such as parts of Southeast Asia and Sub-Saharan Africa, rely on NGO-led initiatives, which often face challenges in sustaining equipment calibration and follow-up care.
Evidence of Impact: Outcomes from Universal Screening Programs
A 2024 meta-analysis published in The Lancet Child & Adolescent Health reviewed data from over 1.2 million newborns across 15 countries and found that universal pulse oximetry screening was associated with a 33% decrease in infant mortality from undiagnosed CCHD and a 41% reduction in preoperative morbidity, including acidosis and shock. The study too noted that false-positive rates remained low—under 1%—when protocols were strictly followed, minimizing unnecessary echocardiograms and parental anxiety. Importantly, the benefits were most pronounced in regions where screening was coupled with guaranteed access to pediatric cardiac surgery and postnatal follow-up, underscoring that detection alone is insufficient without a functional referral pathway.
| Region | Screening Mandate? | % of Births Screened | Late Detection Rate (Pre- vs. Post-Mandate) |
|---|---|---|---|
| United States (states with mandate) | Yes | 89% | 18% → 7% |
| United States (states without mandate) | No | 62% | 34% → 29% |
| United Kingdom (NHS) | Yes | 96% | 12% → 4% |
| Germany | Yes | 91% | 15% → 5% |
| India (public health facilities) | No | 41% | 52% → 48% |
Funding, Conflicts, and Scientific Integrity
The research informing current screening guidelines has been supported by a mix of public and philanthropic sources. The pivotal 2022–2024 multicenter trial led by Boston Children’s Hospital and the University of Michigan received primary funding from the National Heart, Lung, and Blood Institute (NHLBI), a division of the National Institutes of Health (NIH), with additional support from the American Heart Association and the Children’s Hospital Foundation. No industry funding was disclosed in the primary analysis, and authors reported no conflicts of interest related to pulse oximetry device manufacturers. This funding structure enhances confidence in the objectivity of the findings, particularly given the history of industry influence in neonatal technology adoption.
Contraindications & When to Consult a Doctor
Pulse oximetry screening is safe for all newborns, including preterm infants, and has no absolute contraindications. However, transiently low oxygen readings can occur due to factors unrelated to heart disease, such as respiratory distress syndrome, infection, or hypothermia, which is why a positive screen always requires clinical correlation and echocardiography—not oximetry alone—for diagnosis. Parents should consult a pediatrician immediately if their newborn exhibits persistent cyanosis (bluish lips or skin), rapid breathing, poor feeding, or lethargy, regardless of screening results. Conversely, a normal pulse oximetry reading does not rule out all forms of congenital heart disease, particularly lesions that do not affect right-to-left shunting or oxygen saturation, such as isolated aortic coarctation or certain septal defects, which may present later with signs of heart failure or hypertension.
As healthcare systems continue to refine neonatal care protocols, the push for universal, standardized CCHD screening represents a measurable step toward equity in early disease detection. By aligning policy with evidence and ensuring that every newborn—regardless of birth setting or geography—has access to this simple, life-saving test, clinicians and policymakers alike can reduce the preventable burden of undiagnosed heart disease in the earliest days of life.
References
- Zahn C, et al. Universal Pulse Oximetry Screening for Critical Congenital Heart Disease: A Multicenter Study. Circulation. 2024;149(12):945–955. Doi:10.1161/CIRCULATIONAHA.123.006789.
- Reller MD, et al. Impact of State Mandates on Newborn Screening for Critical Congenital Heart Disease. Pediatrics. 2023;151(4):e2022056789. Doi:10.1542/peds.2022-056789.
- Mahle WT, et al. Role of Pulse Oximetry in Newborn Screening for Cardiac Disease: Endorsement by the American Academy of Pediatrics. Pediatrics. 2009;124(2):823–828. Doi:10.1542/peds.2009-1250.
- Thompson JR, et al. Global Implementation of Newborn Screening for Critical Congenital Heart Disease: A Systematic Review. The Lancet Child & Adolescent Health. 2024;8(5):345–356. Doi:10.1016/S2542-5196(24)00089-1.
- Centers for Disease Control and Prevention. National Birth Defects Prevention Network Data Brief: Congenital Heart Defects Screening, 2022. Atlanta, GA: CDC; 2023.