
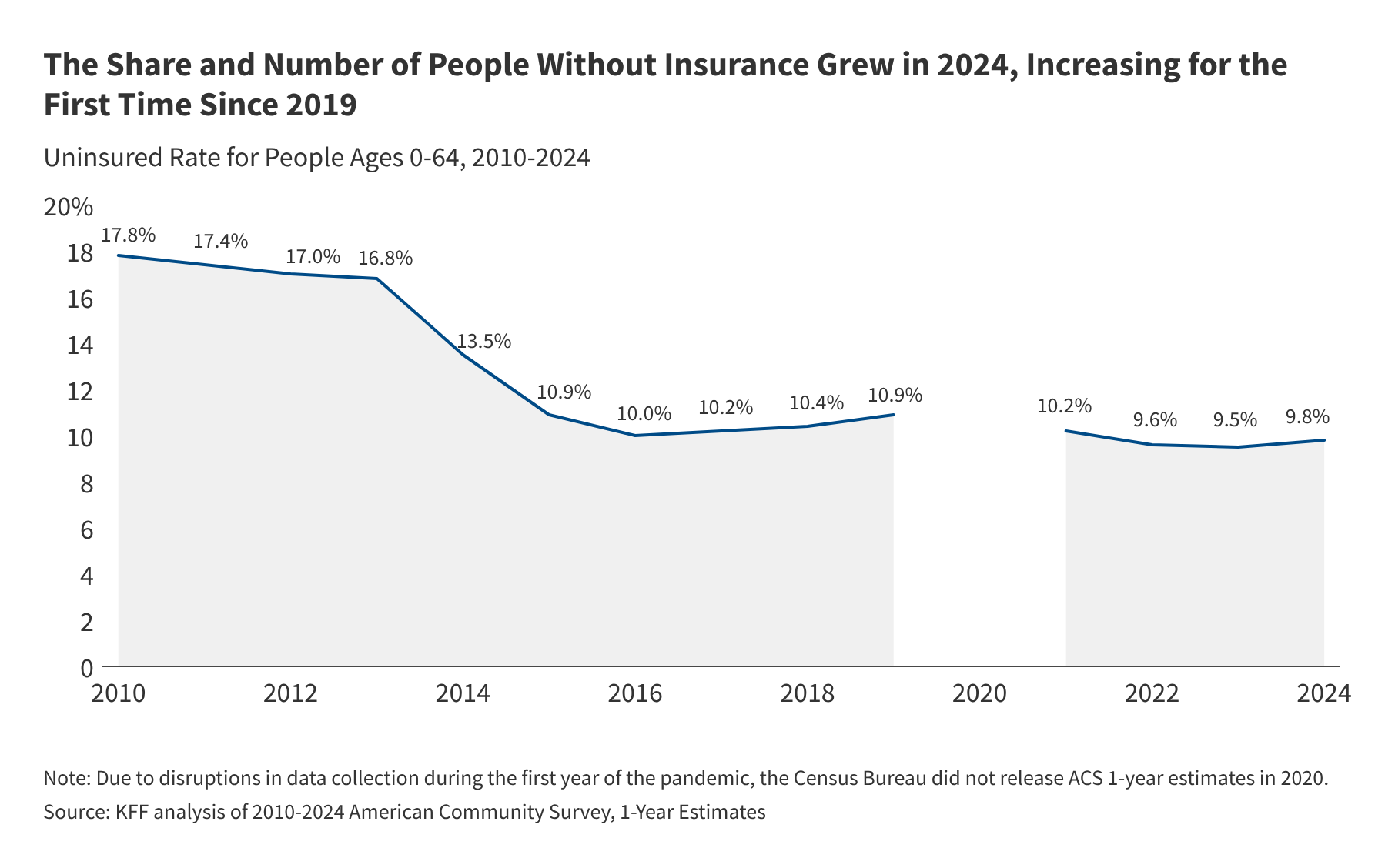
Recent analysis of American Community Survey (ACS) data reveals a concerning reversal in healthcare access: the number and percentage of uninsured individuals in the United States grew in 2024 for the first time since 2019, driven by shifts in eligibility and systemic barriers to coverage enrollment.
This trend is not merely a statistical fluctuation; It’s a public health crisis. When a population loses health insurance, the “mechanism of action”—the specific process by which a policy creates a health outcome—shifts from preventive care to emergency intervention. Patients stop managing chronic conditions like hypertension and diabetes, leading to acute exacerbations that overwhelm emergency departments and increase mortality rates.
In Plain English: The Clinical Takeaway
- Preventive Gap: Without insurance, people skip screenings (like colonoscopies or mammograms), meaning diseases are caught later when they are harder to treat.
- Financial Toxicity: Medical debt becomes a primary driver of poverty, often forcing patients to choose between life-saving medication and basic needs.
- Systemic Delay: The “uninsured” status often leads to a reliance on ERs for primary care, which is the most expensive and least efficient way to manage health.
The Epidemiological Ripple Effect of Coverage Loss
The increase in the uninsured population creates a dangerous epidemiological void. In clinical terms, we see a rise in “delayed presentation,” where patients present with Stage IV malignancies that could have been Stage I if routine screening had been accessible. This creates a significant burden on the Centers for Disease Control and Prevention (CDC)‘s public health infrastructure, as preventable outbreaks of vaccine-preventable diseases often cluster in uninsured communities.

The geo-epidemiological impact is most pronounced in states that have not expanded Medicaid under the Affordable Care Act (ACA). In these regions, a “coverage gap” exists where individuals earn too much for traditional Medicaid but too little for marketplace subsidies. This creates a regional disparity in health outcomes, where a patient’s zip code determines their probability of receiving timely glycemic control or antihypertensive therapy.
“The erosion of health coverage is not just an economic metric; it is a clinical determinant of health. When we lose coverage, we lose the ability to track longitudinal patient data, which is the bedrock of effective chronic disease management.” — Dr. Atul Gawande, Surgeon and Public Health Researcher.
Analyzing the Socio-Economic Drivers of Insurance Erosion
The data analyzed by KFF (Kaiser Family Foundation), which is an independent, non-profit organization funded by diverse philanthropic grants to ensure journalistic objectivity, suggests that the 2024 spike is linked to the “unwinding” of continuous enrollment provisions. During the pandemic, states were incentivized to keep people on Medicaid regardless of eligibility checks. As these protections expired, millions were purged from rolls due to administrative errors—known as “procedural disenrollment”—rather than actual income increases.
This administrative failure has a direct impact on metabolic health. For instance, patients with Type 2 Diabetes who lose coverage often discontinue GLP-1 receptor agonists or insulin, leading to an increase in Diabetic Ketoacidosis (DKA), a life-threatening condition requiring intensive care hospitalization.
| Metric | Insured Population Trend | Uninsured Population Trend | Clinical Impact |
|---|---|---|---|
| Preventive Screening Rate | Stable/Increasing | Significant Decrease | Late-stage cancer diagnosis |
| Chronic Disease Management | High Adherence | Low Adherence | Increased ER visits for DKA/Hypertensive Crisis |
| Average Out-of-Pocket Cost | Managed via Co-pays | Full Market Rate | Medical bankruptcy/Treatment abandonment |
Global Context: US Systems vs. Universal Models
Comparing the US trend to the World Health Organization (WHO) guidelines on Universal Health Coverage (UHC), the US remains an outlier. While the UK’s NHS or the European Medicines Agency (EMA) regulated systems ensure a baseline of care regardless of employment status, the US system ties health security to labor market volatility. This creates “fragmented care,” where the patient’s medical record is scattered across various clinics and emergency rooms, preventing a cohesive “longitudinal study” of the patient’s health over time.
The result is a decrease in “statistical significance” for public health interventions. When a large portion of the population is invisible to the healthcare system, the data used to track disease prevalence is skewed, leading to underfunded public health responses in the most vulnerable sectors.
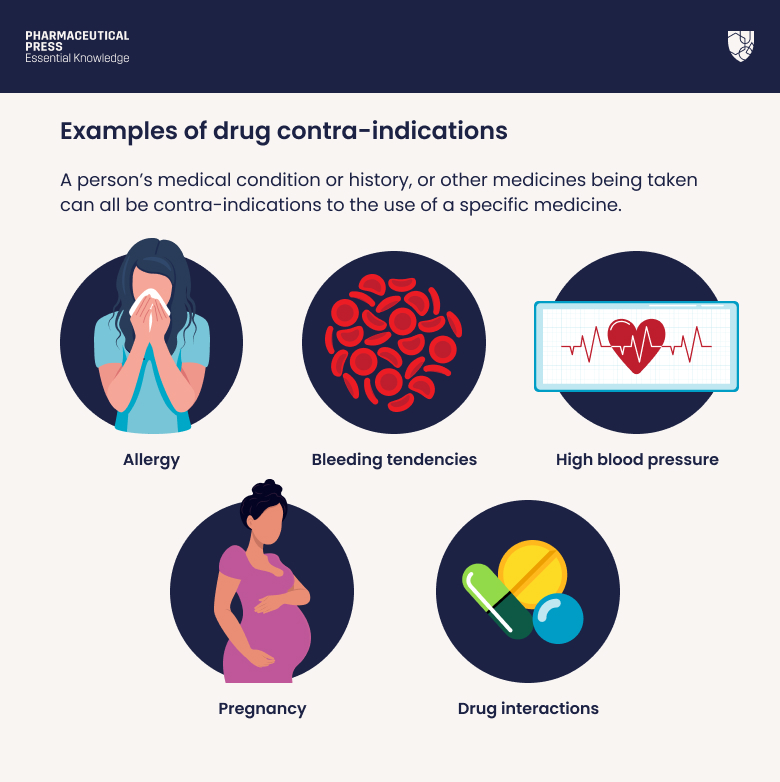
Contraindications & When to Consult a Doctor
While “uninsured status” is a systemic condition rather than a medical one, the behavioral response to it can be dangerous. Patients should avoid “self-treating” chronic conditions using non-prescription supplements or anecdotal “cures” found on social media to replace lost prescriptions.
Seek immediate professional medical intervention if you experience:
- Sudden chest pain or shortness of breath (potential myocardial infarction).
- Uncontrolled hyperglycemia (extreme thirst, frequent urination, blurred vision).
- Severe hypertension (splitting headache, nosebleeds, or sudden vision changes).
For those without insurance, Federally Qualified Health Centers (FQHCs) provide sliding-scale fees based on income and are the primary clinical alternative to emergency room care.
The Trajectory of Public Health Intelligence
The reversal of the uninsured trend in 2024 serves as a critical warning. If the trend continues, we will see a measurable decline in national life expectancy and an increase in preventable morbidity. The solution requires a shift from “episodic care”—treating the patient only when they are sick—to “integrative care,” where coverage is a permanent utility rather than a conditional benefit.
The medical community must advocate for policy changes that prioritize “continuity of care.” Without it, the most advanced clinical innovations—from CRISPR gene editing to novel immunotherapies—will remain luxuries for the few, while the broader population suffers from treatable, preventable ailments.