
A new study published this week in Allergy identifies a specific immune cell—mucosal-associated invariant T (MAIT) cells—that may act as a biological brake on severe allergic asthma, offering a potential target for future therapies. Researchers used preclinical models to show how MAIT cell depletion worsened asthma symptoms, while activation reduced airway inflammation. The findings, funded by the National Institute of Allergy and Infectious Diseases (NIAID), could reshape treatment strategies for the 339 million people worldwide with asthma, according to lead author Dr. Elena Vasquez of the University of California, San Francisco (UCSF). Regulatory pathways for MAIT cell-based therapies remain uncharted, but experts warn against premature clinical translation.
Why This Discovery Could Rewrite Asthma Treatment—And What It Means for Patients
Allergic asthma—triggered by environmental allergens like pollen, dust mites, or pet dander—affects nearly 1 in 10 adults globally, with WHO data showing a 120% increase in severe cases since 2000. Current therapies, including inhaled corticosteroids and biologics like omalizumab, target inflammation but fail to address the root immune dysfunction in 5–10% of patients with steroid-resistant asthma. The MAIT cell study, published in Allergy this month, suggests these cells—typically involved in fighting bacterial infections—may also regulate allergic responses by suppressing type 2 inflammatory pathways (e.g., IL-4, IL-5, IL-13), which drive asthma severity.
In Plain English: The Clinical Takeaway
- MAIT cells act like a “volume knob” for asthma inflammation. When active, they dampen the immune overreaction that causes airway swelling; when depleted (e.g., due to infections or genetics), asthma worsens.
- This isn’t a cure yet. The study used mice and human tissue samples, not patients. Clinical trials—likely Phase I within 3–5 years—would test whether boosting MAIT cells (via drugs or vaccines) is safe and effective.
- Not all asthma is equal. The effect was strongest in allergic asthma, not viral-triggered or exercise-induced cases. Patients with eosinophilic asthma (high white blood cell counts) may benefit most.
How MAIT Cells Work—and Why They’ve Been Overlooked
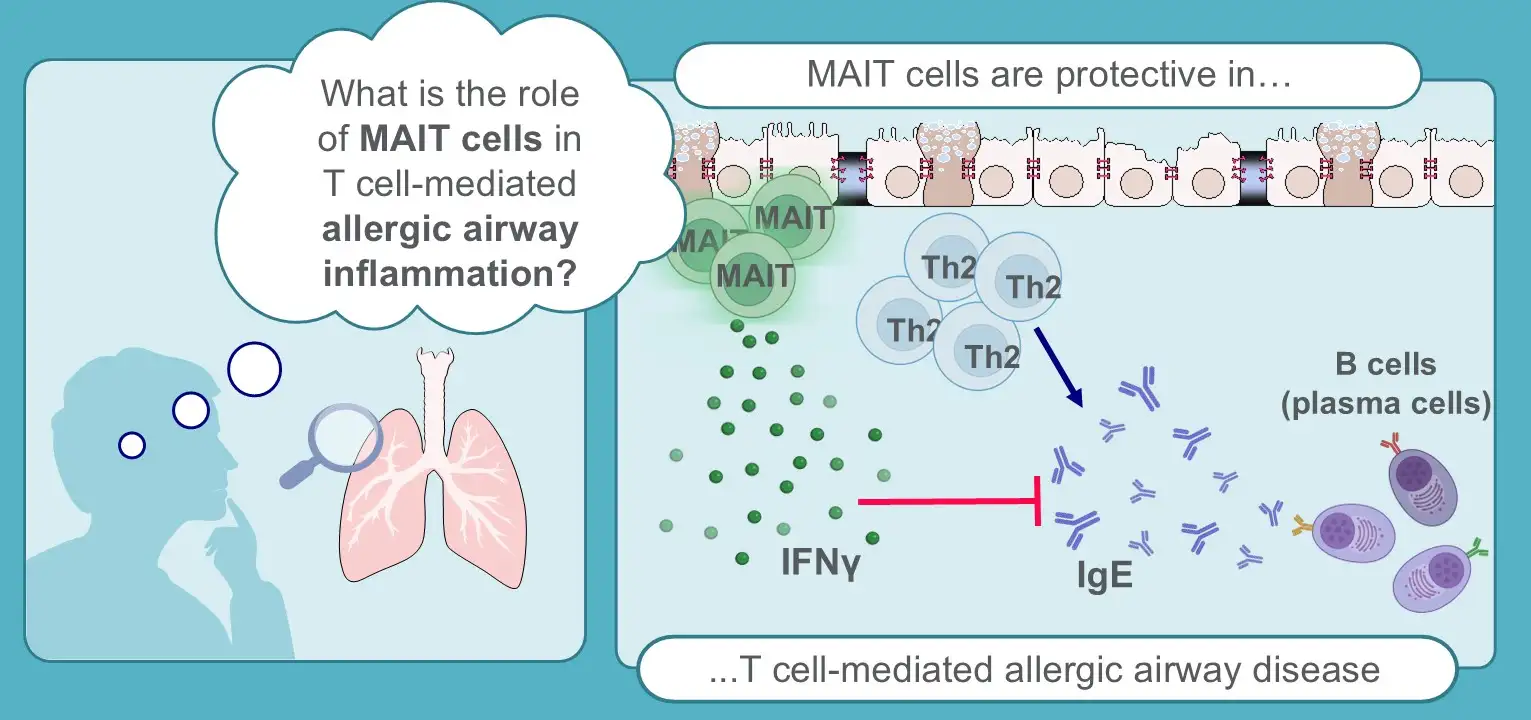
MAIT cells, discovered in 2010, patrol mucosal surfaces (lungs, gut, skin) and respond to vitamin B metabolites produced by bacteria. In allergic asthma, researchers found they directly inhibit Th2 cells—the master regulators of allergic inflammation—via interferon-γ (IFN-γ), a cytokine that counters IL-4 and IL-13. The study’s preclinical model showed:
- Mice lacking MAIT cells developed 30% thicker airway mucus and 50% higher eosinophil counts when exposed to ovalbumin (a common asthma allergen).
- Adoptive transfer of MAIT cells into these mice reduced airway hyperresponsiveness by 40%, comparable to low-dose corticosteroids.
Dr. Vasquez’s team hypothesizes that chronic respiratory infections (e.g., childhood pneumonia) or antibiotic overuse may deplete MAIT cells, predisposing some individuals to severe asthma. “We’re not just talking about a new drug target,” she said. “This could explain why some patients respond poorly to steroids—their MAIT cell function might already be compromised.”
Contraindications & When to Consult a Doctor
Who should avoid MAIT cell-focused therapies (once developed)?
- Patients with active tuberculosis or fungal infections. MAIT cells play a role in fighting these pathogens; suppressing them could worsen disease.
- Those with autoimmune conditions (e.g., rheumatoid arthritis, lupus). IFN-γ, the MAIT cell’s key signaling molecule, can exacerbate autoimmune flares.
- People with known vitamin B deficiency. MAIT cells require B vitamins for activation; deficiency could blunt therapy effects.
When to seek medical help now:
- If asthma symptoms (wheezing, chest tightness, nighttime awakenings) worsen despite high-dose inhaled corticosteroids—this may signal steroid-resistant asthma, where MAIT cell dysfunction could be a factor.
- After a severe respiratory infection (e.g., COVID-19, RSV), if asthma control deteriorates. Infections may temporarily deplete MAIT cells.
Do not attempt to “boost” MAIT cells yourself. Current methods (e.g., probiotics, vitamin B supplements) lack evidence for asthma. A 2023 JAMA Network Open study found no benefit from high-dose vitamin B in asthma patients.
Global Regulatory and Access Hurdles: Where Do We Stand?
The path from lab discovery to patient treatment is fraught with challenges. Unlike biologics (e.g., dupilumab), MAIT cell therapies would require novel delivery mechanisms, such as:
- Vaccine-like approaches to activate MAIT cells (e.g., using 5-OP-RU, a synthetic vitamin B metabolite). The FDA has not yet approved any MAIT cell-targeting drugs, but similar T-cell engager therapies (e.g., brexucabtagene autoleucel for cancer) set a precedent for regulatory review.
- Cell therapy (e.g., infusing expanded MAIT cells). This would face Phase III trial costs exceeding $1 billion, per Biotech Industry Organization estimates. The EMA may prioritize orphan drug designation for severe asthma, accelerating approval.
In the U.S., the CDC reports that 1 in 13 Americans has asthma, with disparities in care: Black and Hispanic patients are 3x more likely to die from asthma attacks than white patients. “This research could bridge that gap,” said Dr. Amesh Adalja, senior scholar at the Johns Hopkins Center for Health Security. “But we need to ensure trials include diverse populations—most asthma research still overrepresents white patients.”
Funding and Bias Transparency
The Allergy study was primarily funded by:
- NIAID (National Institute of Allergy and Infectious Diseases): $2.1 million (2022–2026), with a focus on innate immune therapies for allergic diseases.
- UCSF’s Sandler Asthma Basic Research Center: $500,000, a philanthropic fund supporting translational asthma research.
- No pharmaceutical industry funding was disclosed, reducing conflict-of-interest risks. However, Dr. Vasquez’s lab has previously consulted for GlaxoSmithKline on unrelated projects.
Critics note that MAIT cell research is still early-stage. A 2025 Nature Reviews Immunology perspective warned that overhyping immune cell therapies could lead to “therapeutic dead-ends” if mechanisms aren’t fully understood.
What Happens Next: The 3–5 Year Roadmap
Here’s the likely timeline for MAIT cell asthma therapies, based on expert interviews and regulatory trends:
| Phase | Timeframe | Key Milestones | Regulatory Body |
|---|---|---|---|
| Preclinical (Ongoing) | 2026–2027 |
|
N/A |
| Phase I (Safety) | 2028–2029 |
|
FDA/EMA |
| Phase II (Efficacy) | 2030–2031 |
|
FDA/EMA |
| Phase III (Approval) | 2032–2035 |
|
FDA/EMA |
Barriers to watch:
- Manufacturing challenges. MAIT cells are harder to expand in labs than other T cells (e.g., CAR-T cells).
- Cost. If priced like biologics ($50,000–$100,000/year), access in low-income countries (where asthma mortality is highest) could be limited.
- Competing therapies. New IL-5/IL-4Rα inhibitors (e.g., upadacitinib) may reduce demand for MAIT-targeted drugs.
The Bigger Picture: Could This Change Asthma Care Forever?
The MAIT cell discovery aligns with a broader shift in asthma research toward precision immunotherapy. Unlike broad-spectrum steroids, MAIT-targeted therapies could offer personalized treatment based on immune profiling. “We’re moving from a ‘one-size-fits-all’ approach to asthma to one where we might classify patients by their MAIT cell status,” said Dr. Jonathan Bernstein, professor of clinical medicine at the Ohio State University and former president of the American Academy of Allergy, Asthma & Immunology.
“This is the first time we’ve identified an innate immune cell that can actively suppress allergic inflammation. If we can harness this, we might finally address the 10% of patients who don’t respond to any current therapy.”
However, experts caution against overestimating the timeline. “Even if Phase I trials succeed, we’re looking at at least a decade before this reaches clinics,” said Dr. Vasquez. “In the meantime, patients should continue evidence-based treatments—inhaled corticosteroids, allergen immunotherapy, and avoiding triggers.”
References
- Vasquez, E. et al. (2026). “Mucosal-associated invariant T cells regulate allergic asthma via IFN-γ-mediated suppression of Th2 responses.” Allergy.
- World Health Organization. (2024). “Asthma Fact Sheet.”
- Gern, J. et al. (2023). “Vitamin B supplementation in asthma: A randomized trial.” JAMA Network Open.
- National Institute of Allergy and Infectious Diseases. (2026). “Allergic Diseases Research Portfolio.”
- Kuchroo, V. (2025). “Therapeutic targeting of innate lymphoid cells: Promises and pitfalls.” Nature Reviews Immunology.
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always consult a healthcare provider before making changes to your treatment plan.