
Basal cell carcinoma (BCC), a common form of skin cancer, has been identified in a rare digital presentation following a patient’s report of a non-healing lesion on the finger. While BCC typically occurs on sun-exposed areas like the face, clinicians highlight that chronic, persistent sores on extremities require biopsy to rule out malignancy.
In Plain English: The Clinical Takeaway
- Persistent lesions are red flags: Any sore, bump, or patch of skin that does not heal within four weeks should be evaluated by a dermatologist, regardless of its location.
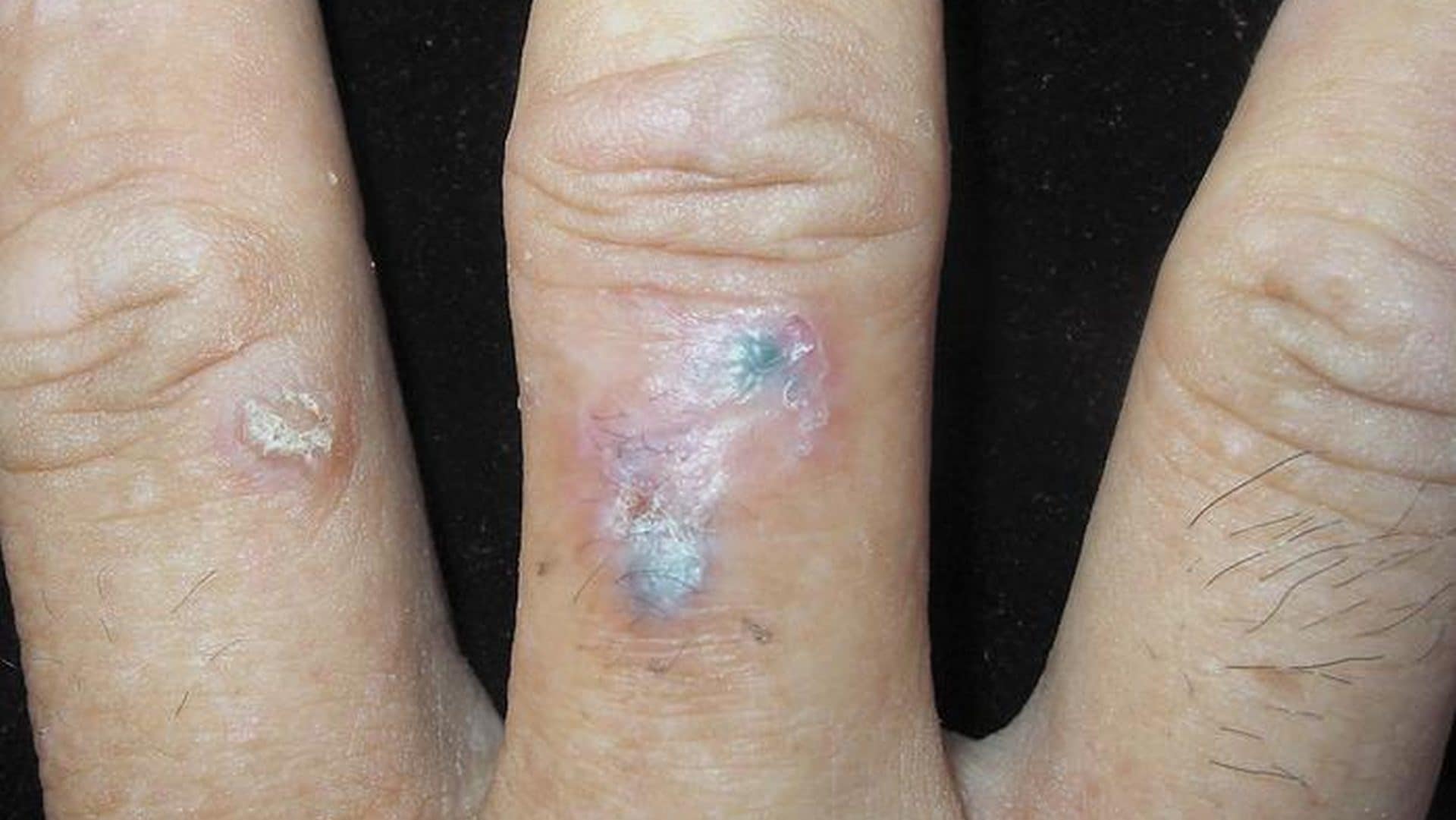
- Digital BCC is an outlier: While BCC is the most frequent skin cancer, its appearance on the fingers or toes is rare and can be mistaken for benign conditions like warts or chronic infections.
- Biopsy is the gold standard: Visual inspection is insufficient for diagnosis; a tissue sample (biopsy) is the only way to confirm if a lesion is cancerous or inflammatory.
Understanding the Mechanism of Digital Basal Cell Carcinoma
Basal cell carcinoma originates from the basal cells—small, round cells found in the lowest layer of the epidermis. According to the American Academy of Dermatology, the primary driver for BCC is cumulative ultraviolet (UV) radiation exposure, which induces mutations in the PTCH1 gene within the Hedgehog signaling pathway. This pathway is a critical regulator of cell growth and differentiation; when dysregulated by UV damage, it triggers uncontrolled cellular proliferation.
While most BCCs emerge on the head and neck, digital (finger) cases represent a unique clinical challenge. Because the digits have a smaller surface area and are often subject to trauma or occupational wear, these tumors are frequently misdiagnosed as paronychia (nail bed infection) or common warts. This delay in diagnosis can lead to deeper invasion into the underlying soft tissue or bone, though metastasis—the spread of cancer to distant sites—remains exceedingly rare for this tumor type.
Clinical Comparison: Presentation and Diagnosis
The following table outlines the differences between standard BCC and the rarer digital presentation identified in clinical literature.
| Feature | Common BCC (Face/Neck) | Digital BCC (Fingers/Toes) |
|---|---|---|
| Primary Etiology | Cumulative UV exposure | UV exposure; potential mechanical trauma |
| Diagnostic Delay | Low (high visibility) | High (mimics benign conditions) |
| Invasive Potential | Locally aggressive | Higher risk of bone/tendon involvement |
| Treatment | Excision/Mohs surgery | Wide local excision/Amputation (if advanced) |
Regulatory Oversight and Patient Access
In the United States, the FDA monitors skin cancer treatments through established protocols for surgical and topical therapies. In Europe, the EMA provides similar regulatory guidance. Patients concerned about persistent finger lesions should utilize primary care networks to obtain a referral to a board-certified dermatologist. Early detection allows for outpatient surgical excision, which carries a high cure rate and avoids the need for more complex reconstructive procedures.
Dr. Elizabeth Billingsley, a leading dermatologic surgeon, notes: `Patients often dismiss a sore on the finger as an injury that hasn’t quite healed. However, when a lesion persists, we must move beyond clinical suspicion and utilize histopathology to ensure we are not missing a basal cell or squamous cell carcinoma.`
Contraindications & When to Consult a Doctor
There is no “treatment” for a non-healing lesion other than professional medical evaluation. Patients should strictly avoid the use of over-the-counter wart removers, topical antibiotics, or herbal salves on undiagnosed, non-healing skin lesions. These substances can mask the clinical appearance of a tumor, potentially delaying a life-saving diagnosis.
You should consult a healthcare provider immediately if you observe a lesion that:
- Bleeds easily or spontaneously.
- Displays a “pearly” or translucent border.
- Has been present for more than one month without signs of resolution.
- Changes color, size, or shape.
The prognosis for localized BCC, even on the digit, remains excellent when treated early. Surgical excision, often performed via Mohs micrographic surgery—a technique where thin layers of skin are removed and examined under a microscope until no cancer cells remain—is the preferred method for ensuring complete tumor clearance while preserving as much healthy tissue as possible.