
2023-07-24 04:18:45
Due to a better understanding of its biologic characteristics, there has been a transition in therapeutic options from chemoimmunotherapy to targeted therapies. However, the latter are not yet curative. They are expensive, have specific toxic effects, and ultimately lead to the development of resistant tumor cell clones. Therefore, clinicians are faced with an increasing number of patients with resistant disease. This is particularly the case where resistance to Bruton tyrosine kinase (BTK) inhibitors develops, usually through the acquisition of a somatic variant that changes the binding site of the protein.
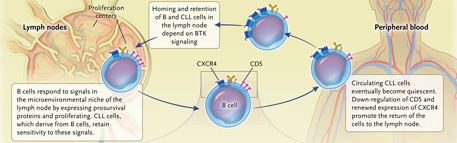
Despite their malignant nature, CLL cells retain sensitivity to external signals in the lymph nodes: in this sense, they resemble healthy, mature B cells. Numerous signals from the microenvironment jointly orchestrate the increased expression of “pro-survival proteins” and the activation and proliferation of malignant B cells. As such, the environment of lymphoid tissues, such as the lymph nodes and spleen, provide a protective niche for CLL cells, and their recirculation between the blood and lymphoid tissue is a fundamental component of the homeostasis of the condition.
BTK is a nonreceptor tyrosine kinase that is a component of the signal transduction pathway that mediates the response of B cells to find their antigen. Its activation is essential for the localization and retention of healthy B cells and also LLC cells in lymphoid tissues. In fact, upon binding of the B cell receptor (BCR) to the CLL cell surface, a signaling cascade is initiated that leads to changes in gene expression that drive proliferation and survival (Figure 1). BTK is a downstream component of the BCR pathway and has a critical role in maintaining the LLC. Because BTK is critical only for B cells, and loss of function is not lethal to the host, it represents an attractive therapeutic target since its inhibition must be specific for B cell inhibition. Deletion of BTK in the LLC cell does not result in immediate cell death, but deprives the LLC cell of proliferative and survival signals.
Figure 1: Bruton’s tyrosine kinase inhibitors in chronic lymphocytic leukemia.
The introduction of covalently bound BTK inhibitors (ibrutinib, acalabrutinib, tirabrutinib, and zanubrutinib) has substantially improved the treatment and prognosis of advanced CLL. Administered as a daily oral drug, the BTK inhibitor causes rapid clinical responses and improvements in quality of life, although cure remains elusive. The response to BTK inhibitors is initially accompanied by an increase in lymphocyte count, reflecting the loss of localization of LLC cells in lymph nodes and perhaps other lymphoid tissues. In patients with recurrent and heavily pretreated disease, BTK inhibitors are associated with a median progression-free survival of 3 to 4 years. As first-line therapy, treatment with a BTK inhibitor produces remissions lasting more than 4 years in approximately 80% of patients.
However, a considerable number of those receiving these agents discontinue therapy due to side effects, which are mostly caused by inhibition of kinases other than BTK. The most common adverse events leading to discontinuation of treatment are cardiac arrhythmias, particularly atrial fibrillation, and pneumonia. Additionally, 13 to 37% of patients discontinue these BTK inhibitors due to loss of efficacy and development of resistance. Discontinuation of a BTK inhibitor due to toxic effects is more common in those receiving ibrutinib, whereas discontinuation due to development of resistance occurs with any of the BTK inhibitors.
All approved BTK inhibitors bind covalently to the cysteine residue (Cys481) within the ADP-binding pocket of the BTK protein, resulting in complete suppression of its activity. The binding is irreversible and can be “overcome” only by the generation of new BTK proteins by the cell. An inevitable consequence of continued inhibition is the development of somatic variants in BTK that reduce the activity of these inhibitors. The most common variants directly affect the Cys481 residue, leading to reversible and unstable binding between BTK and its inhibitors. Less common are acquired “gain-of-function” variants in the gene encoding downstream PLCγ2 kinase (PLCG2). These result in prolonged BCR signalling, occurring alone or in combination with BTK variants.
Non-covalent binding inhibitors do not require Cys481 to bind. Rather, they bind via hydrogen, ionic bonding, and hydrophobic interactions in a reversible manner to the ADP-binding pocket. Although pirtobrutinib is active in patients with Cys481 variants, other variants have been shown to be associated with loss of binding of both classes of inhibitors (covalent and non-covalent), so it is possible that the efficacy of non-covalent inhibitors is also limited by certain somatic variants that occur in BTK.
Other non-covalent BTK inhibitors (eg, nemtabrutinib, fenebrutinib, and vecabrutinib) are in development, but how well they will treat tumors with resistance mutations (other than Cys481) has not yet been determined. A new class of drugs that leads to the destruction of the BTK protein is being evaluated in clinical trials. These BTK degraders induce proteasomal degradation of BTK proteins and appear to work well once morest CLL regardless of variant status.
Time-limited combination therapy is another approach. The idea is to avoid resistance that arises in response to prolonged exposure to the drug. The results support the safety of pirtobrutinib, making it a candidate for new combination therapies to treat chronic lymphocytic leukemia. BTK inhibitors, such as pirtobrutinib, might also be combined with bispecific T-cell antibodies, an approach that should overcome the acquired T-cell dysfunction that occurs in CLL and makes T-cell-directed therapies difficult.
bibliographical source
Inhibiting BTK in Chronic Lymphocytic Leukemia
Arnon P. Kater, M.D., Ph.D., and Barbara Eichhorst, M.D.
Department of Hematology, Cancer Center Amsterdam, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam (A.P.K.); and Department I of Internal Medicine and Center for Integrated Oncology Aachen, Bonn, Cologne, Düsseldorf, University of Cologne, Cologne, Germany (B.E.).
N Engl J Med 2023; 389:83-86
1690175645
#SAVALnet #Science #Medicine